Table 1. Non-pathological causes of blur |
||
The borders of the nodule might be indistinctive for non-pathological causes. First, the echogenicity of a lesion might be similar or even identical to the surrounding non-lesional tissue which could be either the normal thyroid parenchyma or the extrathyroidal tissue in lesions located at the border of the thyroid. The pathognomonic feature of a macrocalcification is the dorsal acoustic shadow. Occasionally this shadow interferes with the borders of the nodule. Improper focusing is the next cause of non-pathological blur. This occurs if we move the transducer too fast or if the patient swallows during the examination.
Benign nodular goiter (cytology) - case 2026 |
|
 |
 |
 |
 |
|
|
Benign nodular goiter (cytology) - case 2104 |
|
 |
 |
|
|
Benign nodule (cytology) - case 2127 |
|
Transverse scan |
Longitudinal scan |
 |
 |
 |
 |
|
|
Benign lesion (cytology) - case 2019 |
|
Transverse scan |
Longitudinal scan |
 |
 |
 |
 |
|
|
Papillary carcinoma (histology) - case conp040 |
|
|
Transverse scans |
|
 |
 |
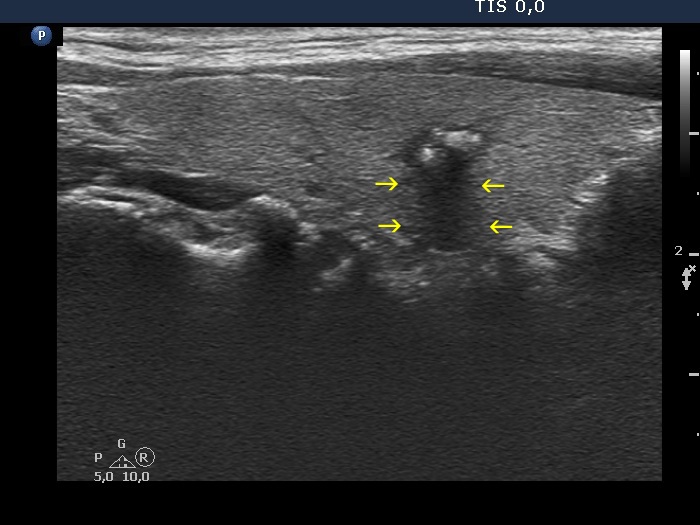
The region of the dorsal border between the two arrows is suspicious being blurred. On the other hand, the echogenicity of the nodule and the extranodular parenchyma are very similar, therefore it is equivocal whether the area in question should be held abnormal. |
|
Papillary carcinoma (histology) - case conp004 |
|
Transverse scan |
Longitudinal scan |
 |
 |
 |
 |
|
|
Papillary carcinoma (histology) - case conp018 |
|
Transverse scan |
Longitudinal scan |
 |
 |
 |
 |
|
|
Benign nodule (cytology) - case 2166 |
|
Transverse scan |
Longitudinal scan |
 |
 |
 |
 |
|
|
Papillary carcinoma (histology) - case conp019 |
|
Transverse scan |
Longitudinal scan |
 |
 |
 |
 |
|
|
Papillary carcinoma (histology) - case conp007 |
|
Transverse scan |
Longitudinal scan |
 |
 |
 |
 |
|
|
Papillary carcinoma (histology) - case conp043 |
|
Transverse scan |
Longitudinal scan |
 |
 |
|
 |
|
|
Bening colloid goiter - case 2119 |
|
Wrong settings |
Right settings |
 |
 |
 |
 |
|
|