
|
|
Study on 100 consecutive patients with thyroid nodule - case 006
|
|







Clinical presentation: A 52-year-old woman was referred for aspiration cytology. She was known harboring a slowly growing nodule in the right thyroid for more than 10 years. She has complaints in recumbent position.
Palpation: a moderately firm nodule in the right lobe.
Functional state: euthyroidism (TSH 1.09 mIU/L).
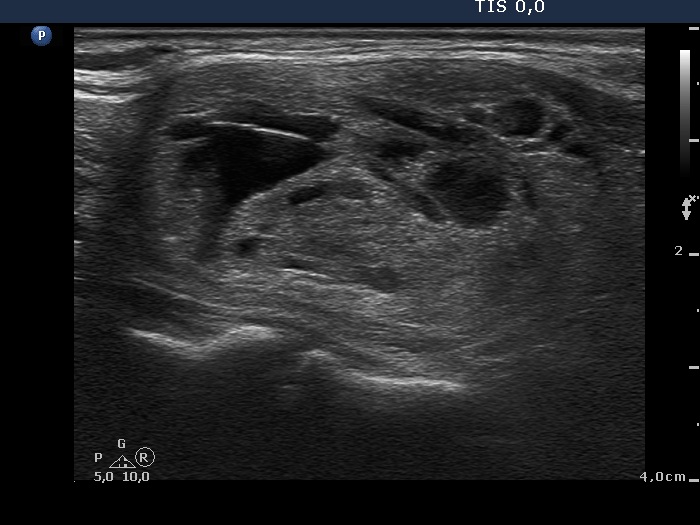
Ultrasonography. The right lobe was composed of a large minimally-moderately hypoechogenic nodule which presented cystic degeneration, halo sign and perinodular blood flow. The left lobe was echonormal and contained small, moderately hypoechogenic areas.
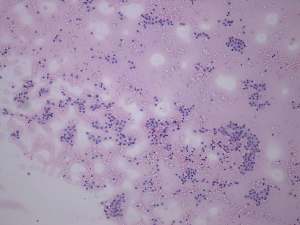
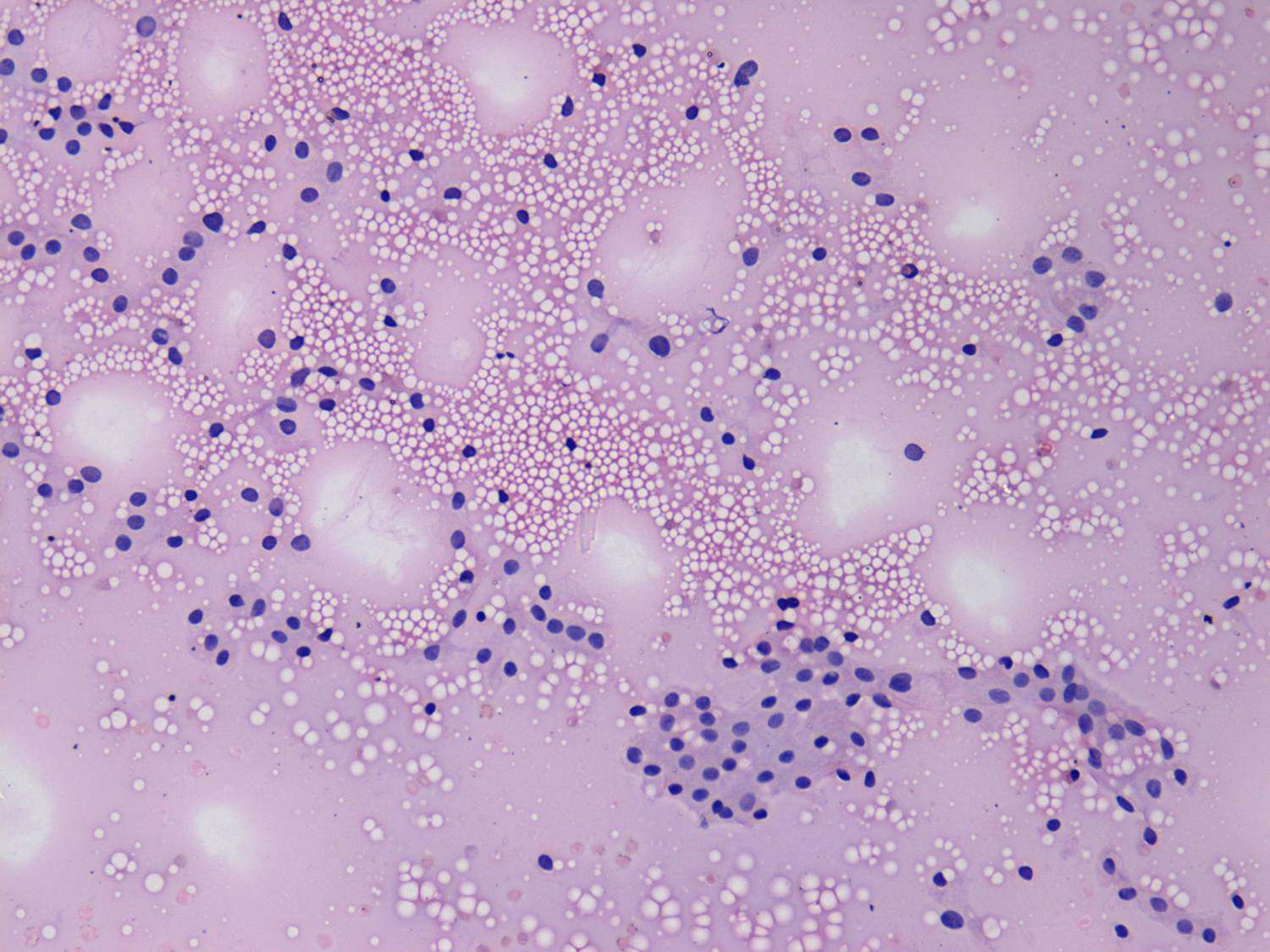
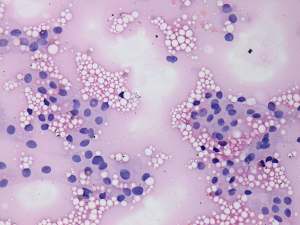
Cytological diagnosis: benign follicular proliferation without significant atypia. There was one atypical cell group on three smears.
Combined cytological-ultrasound diagnosis: follicular tumor with less than the average risk of carcinoma.
Surgery was advised not because of the cytological pattern but because of the compression signs. A right lobectomy was performed. Histopathloogy disclosed follicular adenoma and lymphocytic thyroiditis in the non-nodular part of the lobe.
Comment. This is not a rare finding that we find a few atypical cells or cell groups on microscopic analysis. Common sense is worth following in this case: if we sample from several parts of the nodule and see only one suspicious group of cells, then we have no reason to assume that it is an entirely malignant nodule.