|
Chronic
lymphocytic thyroiditis - Figure 13. Differential diagnostic
problem: Graves' disease or lymphocytic thyroiditis.
Even the clinical and biochemical differentiation between these entites is not simple in significant proportion of cases. It is not surprising because in essence they belong to the same group: autoimmune thyroid disorders. |
CLOSE |
|
Chronic lymphocytic thyroiditis - case 9. |
|
 |
 |
|
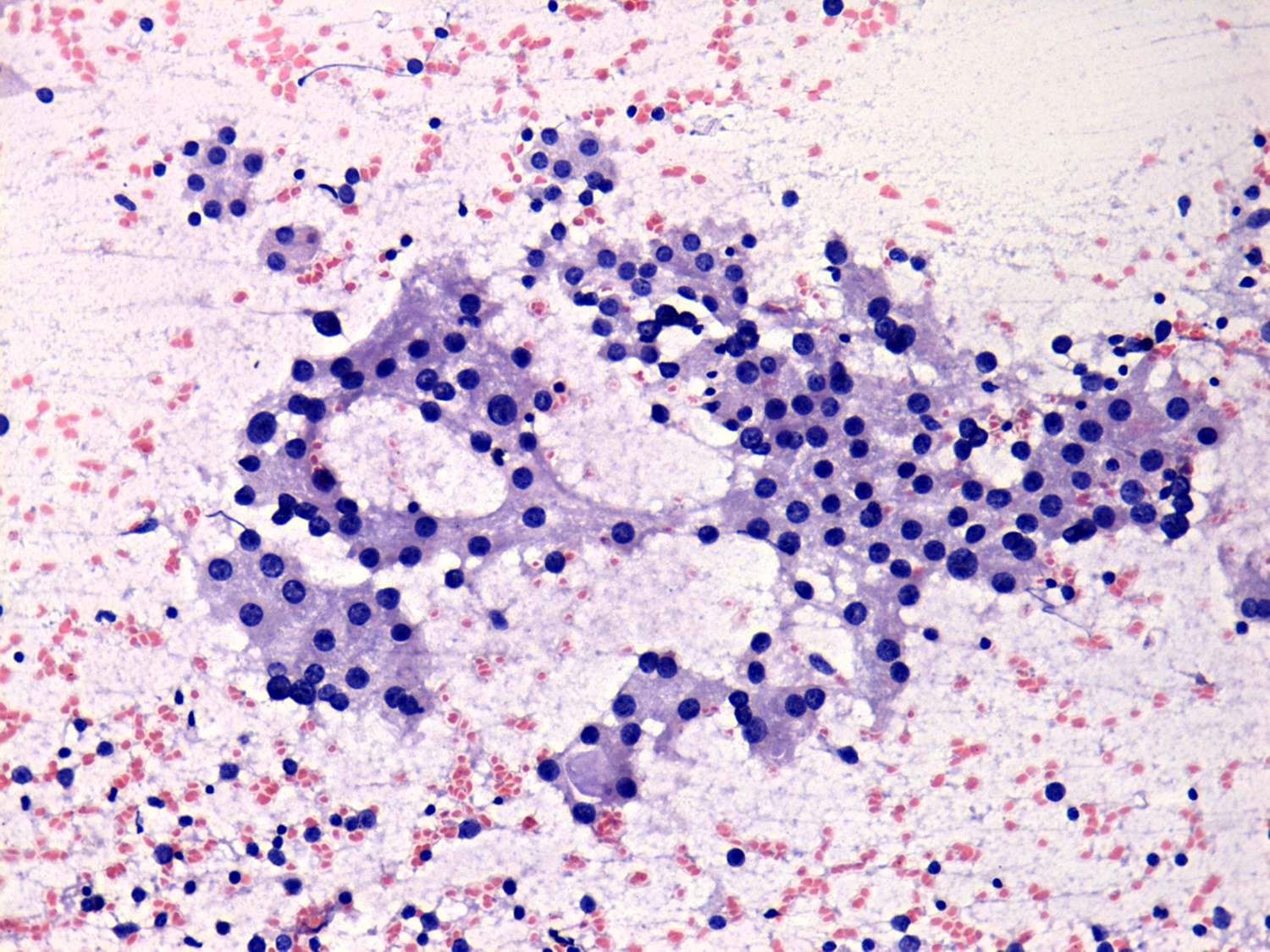
This patient presented with a sublcinical hypothyroidism and a hypoechogenic nodule. The cytological pattern is identical to that seen in an active Graves' disease while the patient had a chronic lymphocytic thyroiditis. The stimulation of thyroid cells either by elevated TSAb in hyperthyroid Graves' disease or elevated TSH in hypothyroidism may cause similar cytological signs, i.e. vacuolization and anisonucleosis. |
|
|
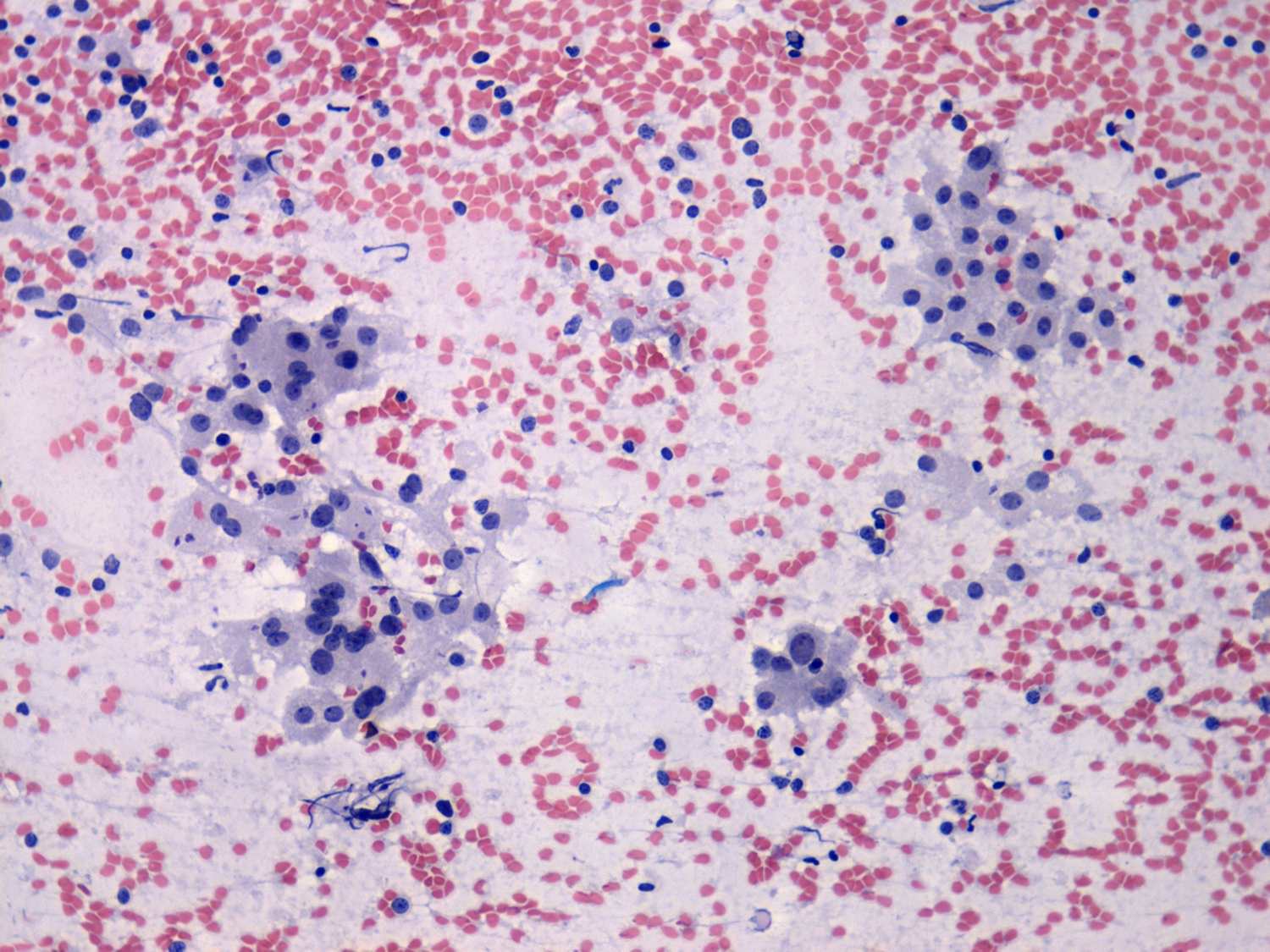
Chronic lymphocytic thyroiditis - case 10 TSH 0 mIU/L, FT4 46.3 pM/L, TSAb 12 U/L. |
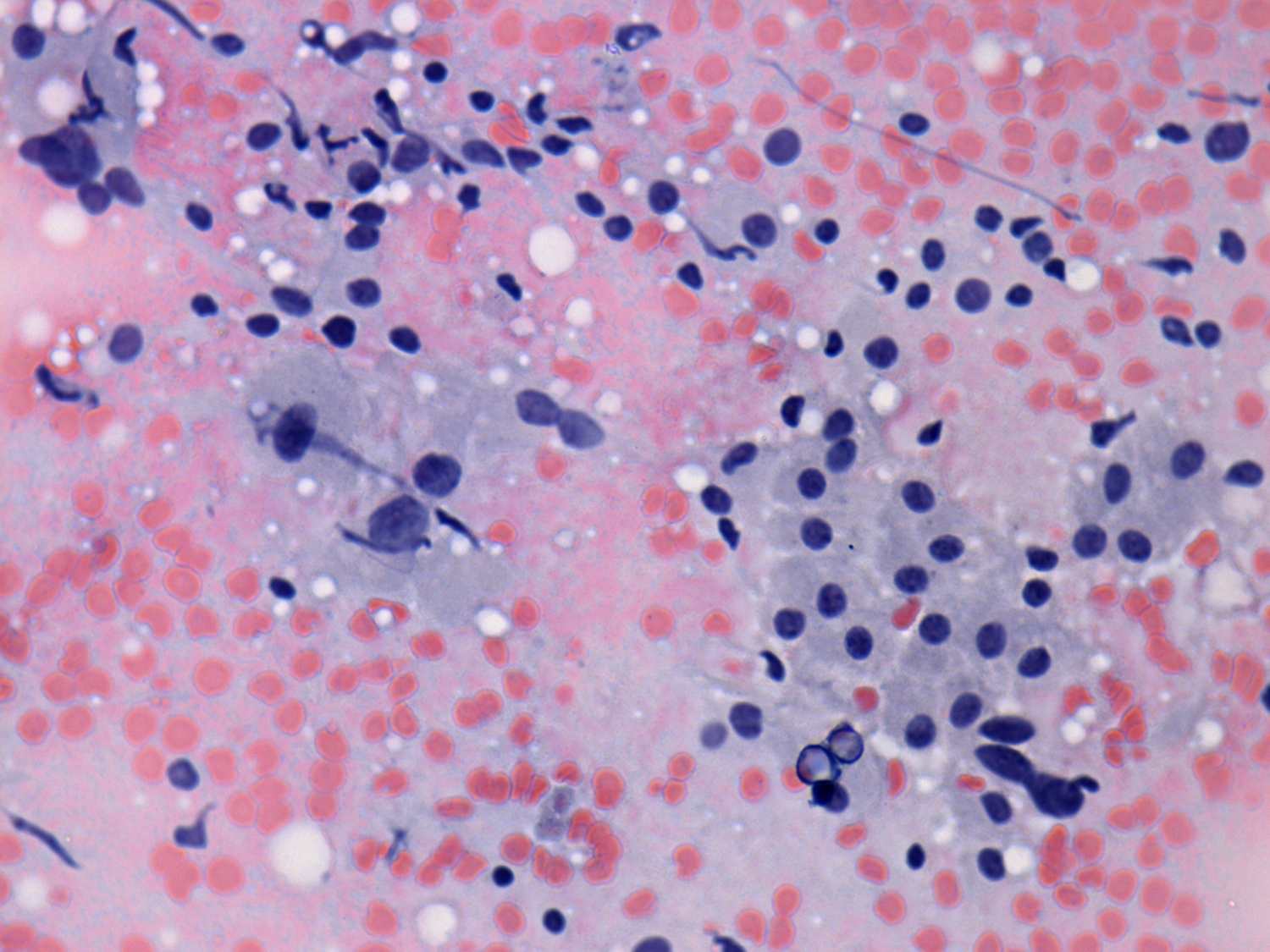
Chronic lymphocytic thyroiditis - case 33 TSH 0 mIU/L, FT4 28.1 pM/L, TSAb 1.1 U/L. |
 |
 |
 |
 |
|
The cytological differentiation may have important role in patients with only mild or moderate hyperthyroidism. In such cases the question is whether the elevated hormon levels are caused by destruction (i.e. thyroiditis) or active hormone producing Graves' disease. In both cases cytology disclosed Hashimoto's thyroiditis. Note the presence of lymphocytes marked with green within the oxyphilic cell group in the lower left image. We did not administer thyrostatics and both patients became euthyroid within weeks after the first investigation. Pay attention that the TSAb was highly elevated in the left case. |
|