
|
|
Benign nodular hyperplasia - cytology |
|
Cytology
Benign colloid goiter is the cytological presentation of a hyperplastic nodule. This is the most common lesion in thyroid cytology and histopathology. Most cases can be diagnosed without difficulty. However, even a low proportion of atypical patterns means a high absolute number of cases involving a differential diagnostic problem. In some of these cases, the combined use of US and FNAC is of importance in order to avoid unnecessary surgery.
Typical pattern
- Colloid in the background.
- The dominant cell-cluster type is a cohesive sheet, forming a honeycomb pattern.
- The dispersed cells have no cytoplasm.
Variants involving minimal diagnostic difficulties
- Cystic degeneration with preserved epithelial cells in the smear.
- (Focal) lymphocytic thyroiditis.
- A number of scattered oncocytes in the smear. Most of the cases with papillarization.
- Atypia: nuclear enlargement and pleomorphism.
Variants involving significant diagnostic difficulties
- Hürthle-cell metaplasia.
- A few cases with papillarization.
- Follicular proliferation.
- Atypia: nuclear pseudoinclusions and grooves.
- Cystic degeneration without preserved epithelial cells in the smear.
BACKGROUND
As mentioned above, most cases of nodular goiters can be diagnosed by FNAC without difficulty. The most important feature favouring the diagnosis is the presence of colloid. A diffuse colloid background practically excludes the possibility of a malignant tumor in the smear. (A review of our false-negative cases revealed no cytological misinterpretation in those cases where a diffuse colloid background could be observed.) The smaller the proportion of colloid in the smear, the greater the chance that a non-characteristic picture will be seen and the greater the chance that a differential diagnostic problem will occur. Detection of the colloid in the smear is greatly influenced by the staining method applied. The major limitation of the Papanicolau method is in this field. The Wright-Giemsa method, and especially the hematoxylin-eosin method, is more suitable for the detection of colloid in the background. TABLE On the other hand, the nuclear details are visualized best with the Papanicolau method, and least well with the hematoxylin-eosin method. Combined use of the Papanicolau method and the Wright-Giemsa method may be of great advantage in this field.
CELLULAR ARRANGEMENT
The most frequent and
most important pattern observed in connection with nodular goiters is
the occurrence of cell clusters of various sizes
and types. Two well-c ircumscribed
patterns may be seen. The first pattern is the honeycomb
arrangement of follicular cells. These are
monolayered sheets without overlapping of the cells. The latter feature
is an important one as concerns a distinction of nodular goiter from
papillary cancer. Nuclear details are relatively well preserved
in the honeycomb cell arrangement. The other pattern is the
ircumscribed
patterns may be seen. The first pattern is the honeycomb
arrangement of follicular cells. These are
monolayered sheets without overlapping of the cells. The latter feature
is an important one as concerns a distinction of nodular goiter from
papillary cancer. Nuclear details are relatively well preserved
in the honeycomb cell arrangement. The other pattern is the papillary
frond. This is a multilayered, three-dimensional
sheet of cells. The nuclear details cannot be interpreted clearly
because of the overlapping of the cells. The edge of these papillae are
not sharp in cases of nodular goiters. Even more important, the
dispersed cells near a papillary cluster
are pyknotic, without cytoplasm. These features are of great help in the correct interpretation of
papillary fronds. This is of great
significance, because the nuclear details within
these multilayered cell clusters are not well preserved. TABLE
papillary
frond. This is a multilayered, three-dimensional
sheet of cells. The nuclear details cannot be interpreted clearly
because of the overlapping of the cells. The edge of these papillae are
not sharp in cases of nodular goiters. Even more important, the
dispersed cells near a papillary cluster
are pyknotic, without cytoplasm. These features are of great help in the correct interpretation of
papillary fronds. This is of great
significance, because the nuclear details within
these multilayered cell clusters are not well preserved. TABLE
Follicular
patterns of various sizes may be observed in most cases of
nodular goiters. One pattern causes no diagnostic problem:
microfollicles aspirated in toto are  three-dimensional structures, which are characteristic
of nodular goiters (Droese 1995). The higher the
proportion of folliculi and the lower the proportion of any other type
of cell clusters, the greater the chance that the lesion is a
follicular tumor rather than a nodular goiter. On the basis of the type
of folliculi (except for the above-mentioned in toto structure) or the
cells forming the folliculi, nodular goiters cannot be distinguished
from follicular tumors. The relative proportion of folliculi and cell
clusters, and the presence or absence of colloid may be indicative
of the given type of lesion.
three-dimensional structures, which are characteristic
of nodular goiters (Droese 1995). The higher the
proportion of folliculi and the lower the proportion of any other type
of cell clusters, the greater the chance that the lesion is a
follicular tumor rather than a nodular goiter. On the basis of the type
of folliculi (except for the above-mentioned in toto structure) or the
cells forming the folliculi, nodular goiters cannot be distinguished
from follicular tumors. The relative proportion of folliculi and cell
clusters, and the presence or absence of colloid may be indicative
of the given type of lesion.
The occurrence of dispersed cells within a thick colloid  background is one
of the most characteristic features in nodular goiters. These
cells may be pykcnotic or enlarged, and they may exhibit
Hürthle-cell metaplasia. In a colloid background, the nuclear
atypia of dispersed cells is of no relevance. Another example is the
above-mentioned occurrence of dispersed cells near papillary fragments.
The characteristic of these cells is of great relevance: in nodular
goiters, these cells are pyknotic, a feature of great help in the
correct interpretation of papillary fronds. Psammoma bodies occur
rarely in smears from nodular goiters, but in these cases the
possibility of papillary cancer must be taken into account (Riazmontazer
1991).
background is one
of the most characteristic features in nodular goiters. These
cells may be pykcnotic or enlarged, and they may exhibit
Hürthle-cell metaplasia. In a colloid background, the nuclear
atypia of dispersed cells is of no relevance. Another example is the
above-mentioned occurrence of dispersed cells near papillary fragments.
The characteristic of these cells is of great relevance: in nodular
goiters, these cells are pyknotic, a feature of great help in the
correct interpretation of papillary fronds. Psammoma bodies occur
rarely in smears from nodular goiters, but in these cases the
possibility of papillary cancer must be taken into account (Riazmontazer
1991).
CELLULAR DETAILS
As regards the nuclear
details, cells from a nodular goiter display great variability. In most
cases, the cells are round, and of uniform size. Nucleoli may be seen
only exceptionally, and they are not prominent or enlarged. If a great
variability in size is observed, this may reflect hormonal
alterations or degenerative changes, including the presence of focal
lymphocytic thyroiditis. Thyrostatic drugs in the history, or isotope
therapy for hyperthyroidism, may cause serious alterations in the nuclei
even some decades later. The nuclei in these cases are
characteristically round, but may be greatly enlarged. As mentioned
above, the presence of pyknotic nuclei is a characteristic feature of
nodular goiters.
nuclei
even some decades later. The nuclei in these cases are
characteristically round, but may be greatly enlarged. As mentioned
above, the presence of pyknotic nuclei is a characteristic feature of
nodular goiters.
The cytoplasm of the cells is not well preserved in the smears. On the
other hand, oncocytic metaplasia is 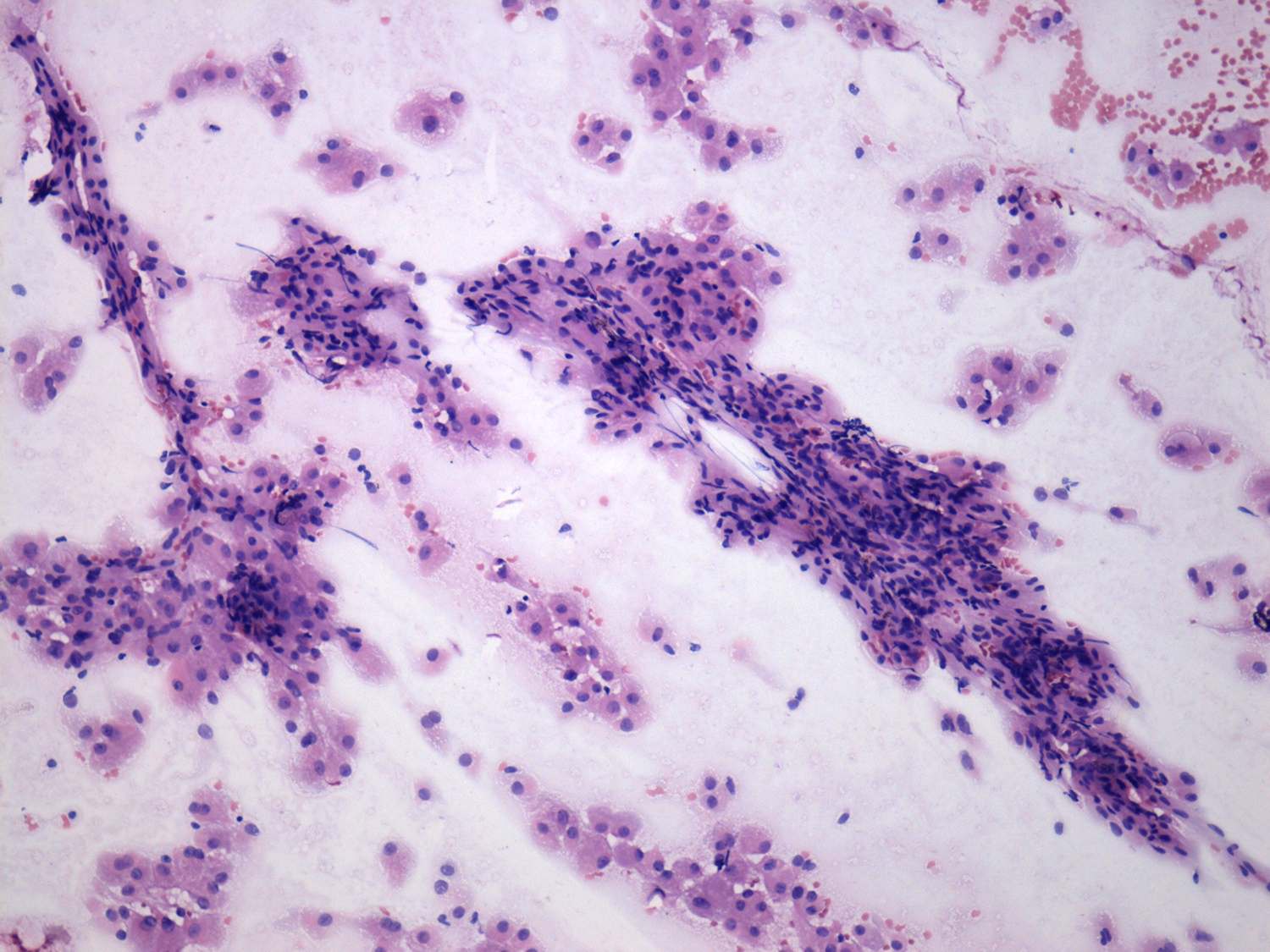 relatively
often observed. In the rare cases where oncocytes are the prominent
cell type, this causes serious interpretation difficulties. The
arrangements of oncocytes, the presence or absence of prominent
nucleoli and the presence or absence of colloid in the background may
be of help. If oncocytes are arranged in regular sheets, nucleoli are
not prominent there is and colloid in the background, the patient can
avoid unnecessary surgery. But if any one of these three features is
missing, the probability of oncocytic tumor is greatly increased.
relatively
often observed. In the rare cases where oncocytes are the prominent
cell type, this causes serious interpretation difficulties. The
arrangements of oncocytes, the presence or absence of prominent
nucleoli and the presence or absence of colloid in the background may
be of help. If oncocytes are arranged in regular sheets, nucleoli are
not prominent there is and colloid in the background, the patient can
avoid unnecessary surgery. But if any one of these three features is
missing, the probability of oncocytic tumor is greatly increased.
Nuclear inclusions and grooves are
relatively infre quent in
cases of nodular goiters. Scattered nuclei (i.e. only 1 or 2 per smear)
with these features may be observed in some cases. This has no relevance.
However, if
the number of cells with these atypia is
higher, the correct interpretation may be
difficult or even impossible. A great proportion of these patients are
sent to surgery with the suspicion of
papillary cancer, and
quent in
cases of nodular goiters. Scattered nuclei (i.e. only 1 or 2 per smear)
with these features may be observed in some cases. This has no relevance.
However, if
the number of cells with these atypia is
higher, the correct interpretation may be
difficult or even impossible. A great proportion of these patients are
sent to surgery with the suspicion of
papillary cancer, and  most of
the cases prove to be nodular goiter with serious degenerative changes.
The other type of this diagnostic problem with nuclear inclusions and
grooves occurs in lesions later proven to be nodular goiter with focal
lymphocytic thyroiditis. The nuclear atypia seen in lymphocytic
thyroiditis is discussed in the relevant chapter. Here, we merely
mention the possibility that in patients with nodular goiters, where
focal lymphocytic thyroiditis also occurs, nuclear grooves can be seen.
Even in cases where a significant number of lymphocytes are visible in
the smear, the correct diagnosis may be difficult. And in cases where
we are not aware of the presence of lymphocytic thyroiditis, the
problem may be more serious.
most of
the cases prove to be nodular goiter with serious degenerative changes.
The other type of this diagnostic problem with nuclear inclusions and
grooves occurs in lesions later proven to be nodular goiter with focal
lymphocytic thyroiditis. The nuclear atypia seen in lymphocytic
thyroiditis is discussed in the relevant chapter. Here, we merely
mention the possibility that in patients with nodular goiters, where
focal lymphocytic thyroiditis also occurs, nuclear grooves can be seen.
Even in cases where a significant number of lymphocytes are visible in
the smear, the correct diagnosis may be difficult. And in cases where
we are not aware of the presence of lymphocytic thyroiditis, the
problem may be more serious.
Cystic degeneration is a very frequent
phenomenon in nodular goiters. In cases where this is only limited and
no cystic fluid can be aspirated, the correct diagnosis is not
difficult: we can see the common picture of nodular goiters, with some
cells with cystic degeneration. On the other hand, one of the most
important limitations of thyroid cytology and one of the most important
differential diagnostic problems in the evaluation of thyroid nodules
is the differential diagnostics and management of thyroid cysts.
The occasional presence of multinucleated giant cells
reflects degenerative changes and is of no relevance. On the other
hand, the presence of even a small number of lymphocytes
should raise the possibility of pre-existing autoimmune lymphocytic
thyroiditis. Solely from the cytological picture, we cannot exclude the
possibility of the latter.
The cytology of nodular goiters treated for hyperthyroidism is
discussed in the relevant chapter.