Table 6. Differential diagnotics of lobulated and spiculated margins |
||
As in many cases of differential diagnostic, the issue is whether an irregular border is caused by any forms of thyroiditis or a pathological nodule. The former is characterized by multiple while the latter with only one or two discrete lesions per thyroid lobe. A clear distinction simply on ultrasound pattern is not infrequently impossible.
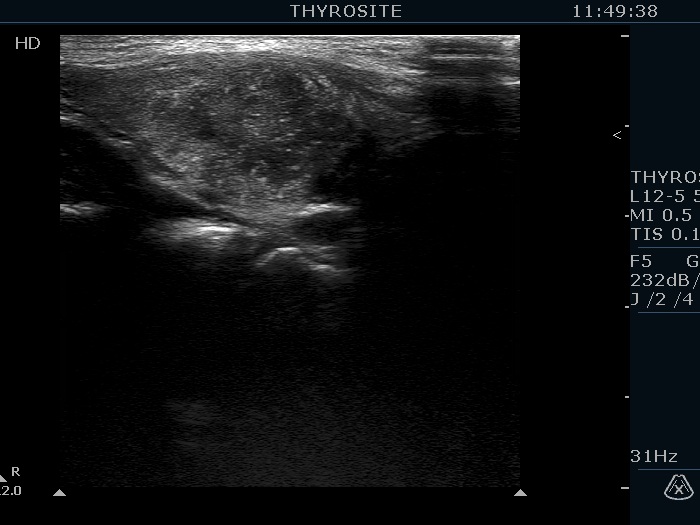
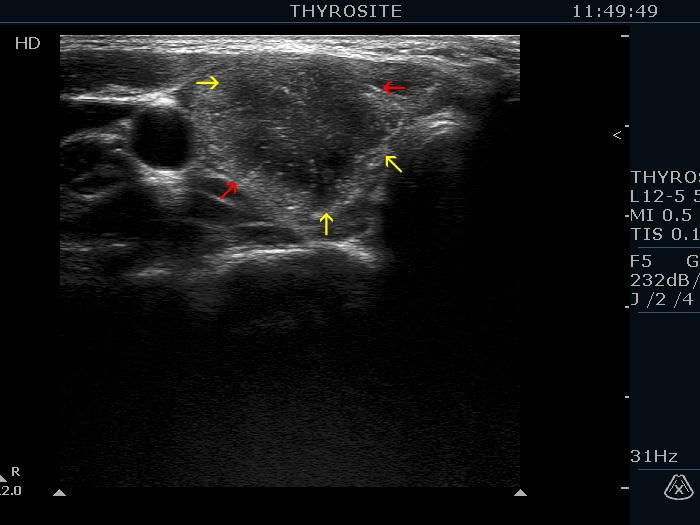
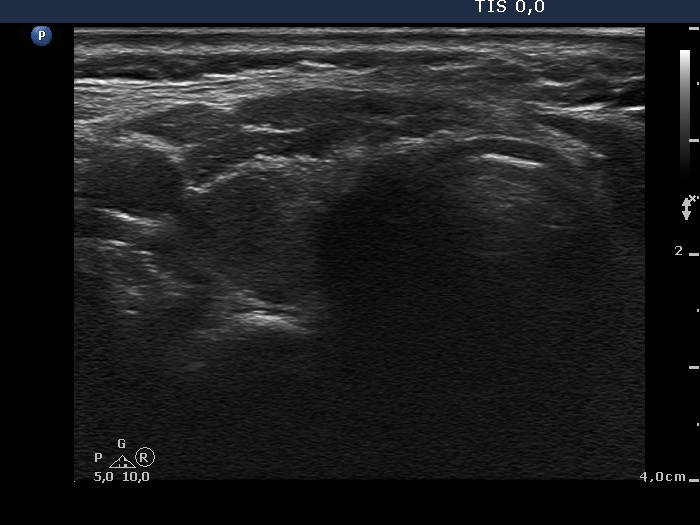
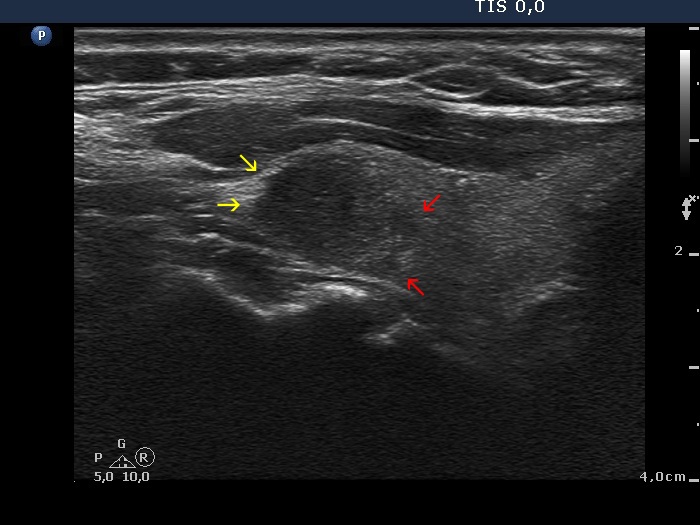
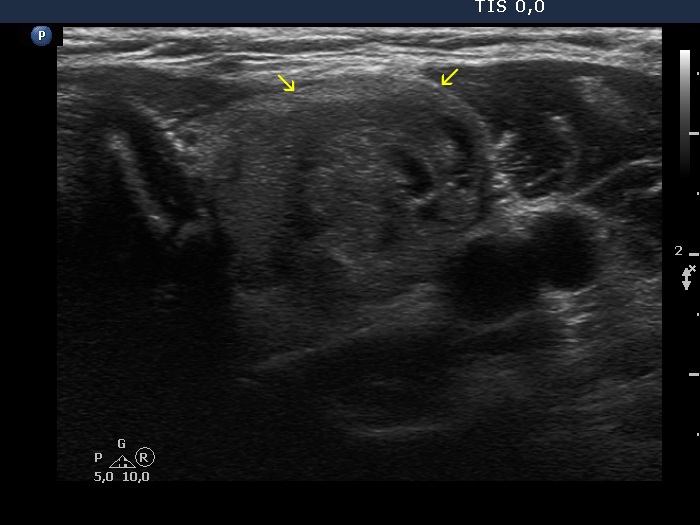
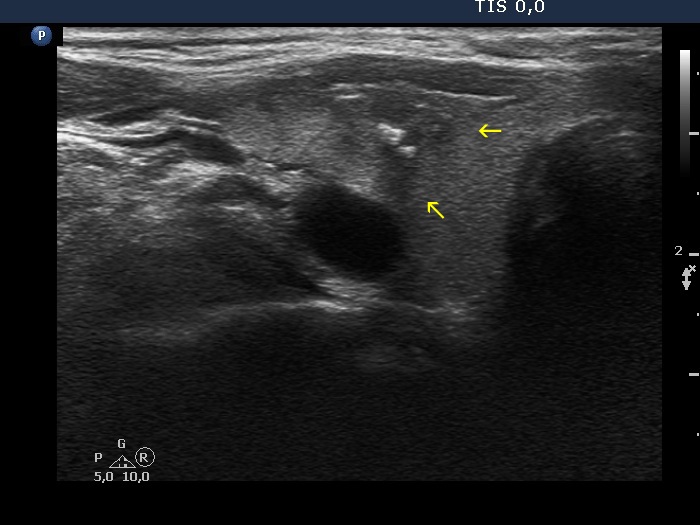
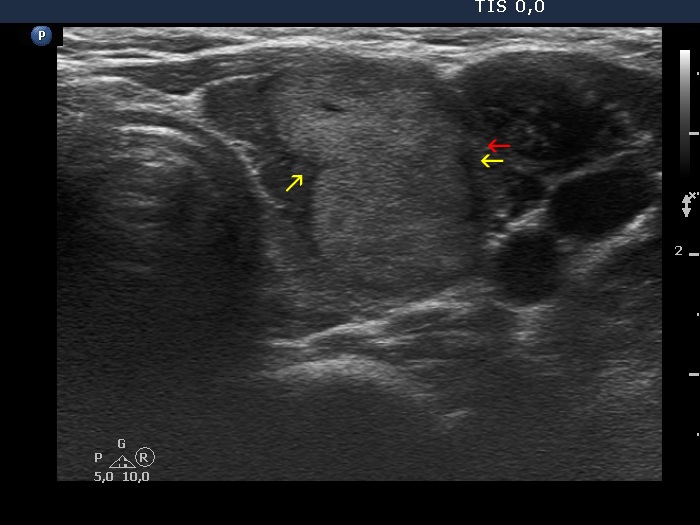
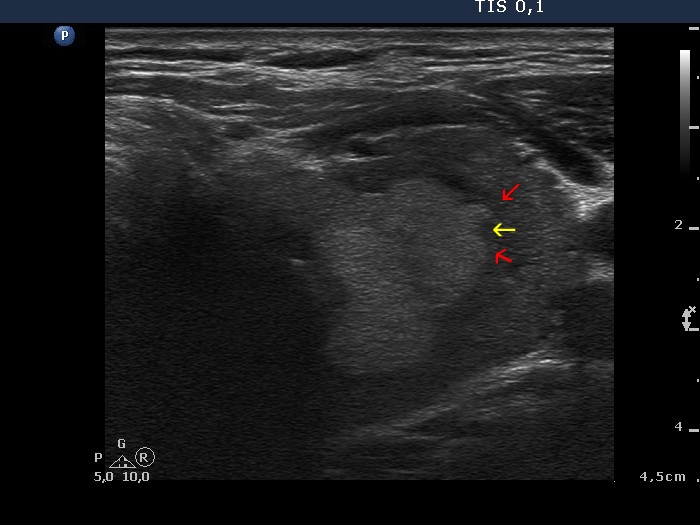
Papillary carcinoma (histology) - case conp003 |
|
Transverse scan |
Longitudinal scan |
 |
|
 |
 |
|
|
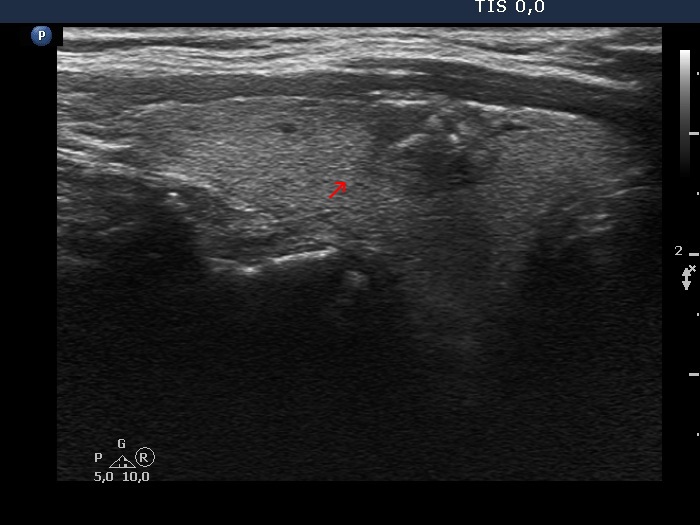
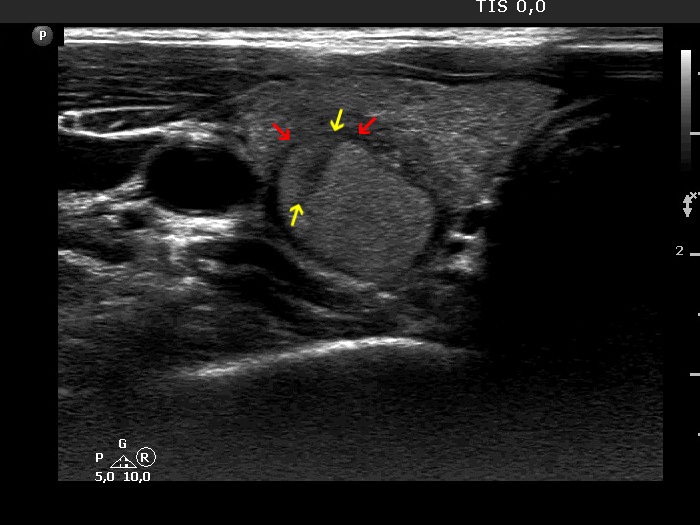
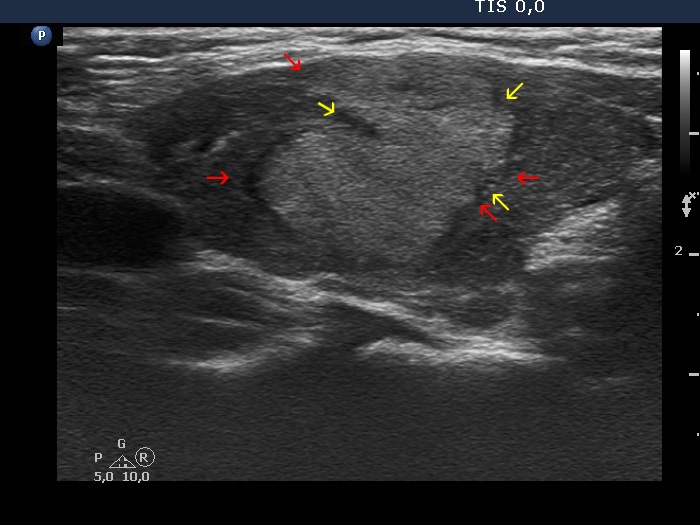
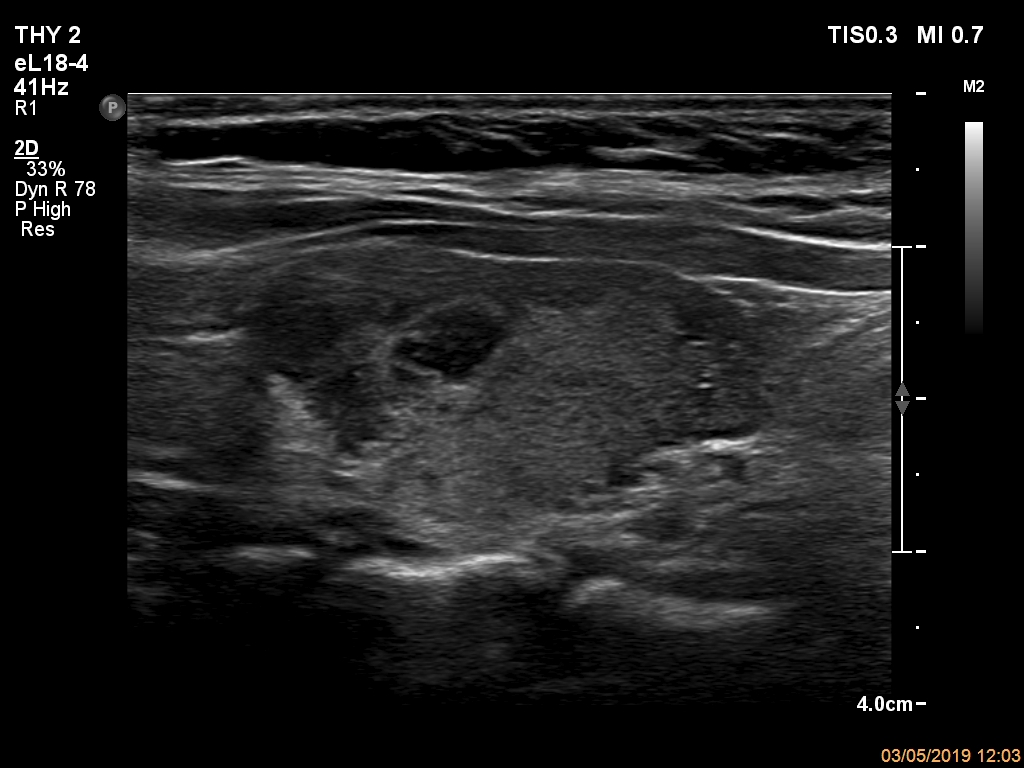
Papillary carcinoma (histology) - case 2082 |
|
Transverse scan |
Longitudinal scan |
 |
 |
 |
 |
|
|
Papillary carcinoma (histology) - case conp009 |
|
Transverse scan |
Longitudinal scan |
 |
 |
|
|
Benign lesion (cytology) - case 2069 |
|
Transverse scan |
Longitudinal scan |
 |
 |
 |
 |
|
|
Papillary carcinoma (histology) - case conp010 |
|
Transverse scan |
Longitudinal scan |
 |
 |
|
|
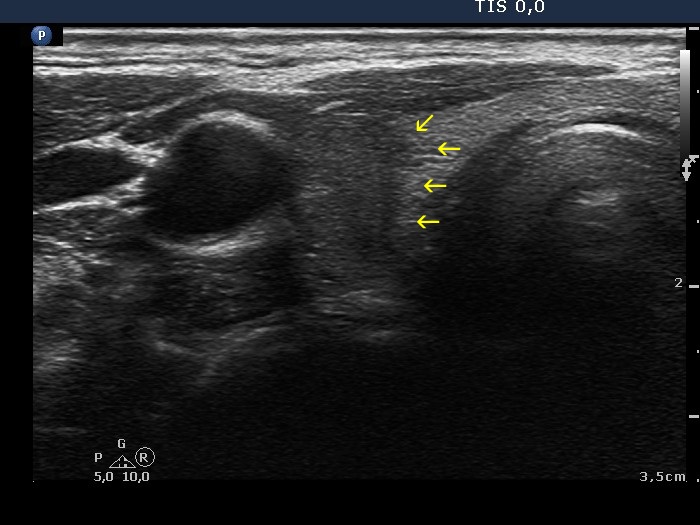
Papillary carcinoma (histology) - case conp051 |
|
Transverse scan |
Longitudinal scan |
 |
 |
 |
 |
|
|
Papillary carcinoma (histology) - case conp020 |
|
Transverse scan |
Longitudinal scan |
 |
 |
 |
 |
|
|
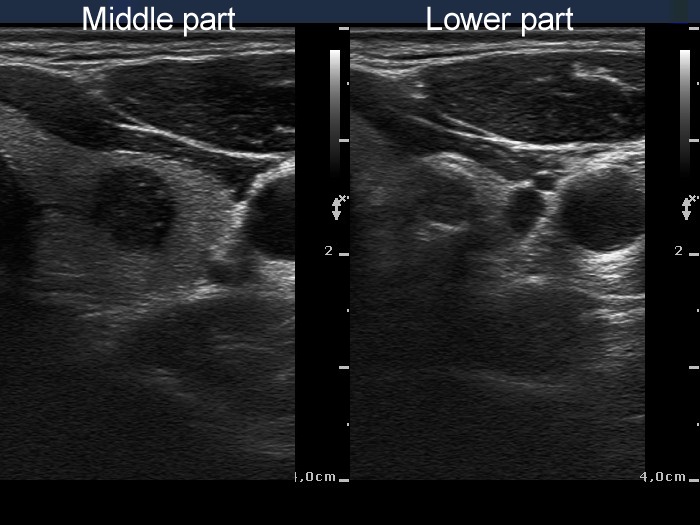
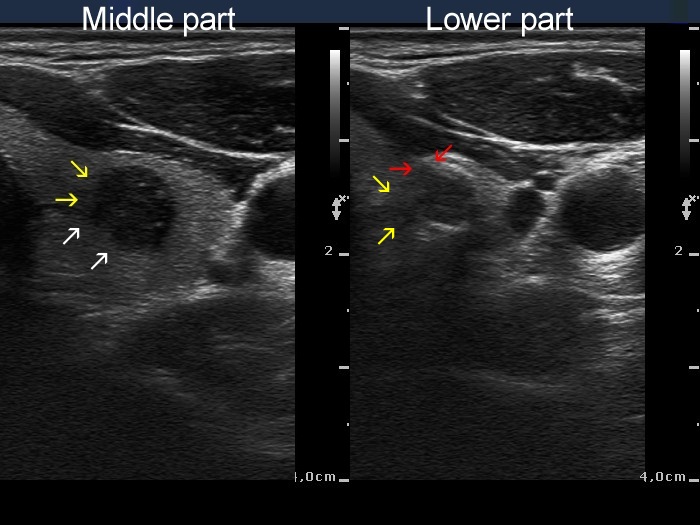
Papillary carcinoma (middle) and benign hyperplastic nodule (lower) (histology) - case conp034 |
|
Transverse scan |
Longitudinal scan |
 |
 |
 |
 |
|
|
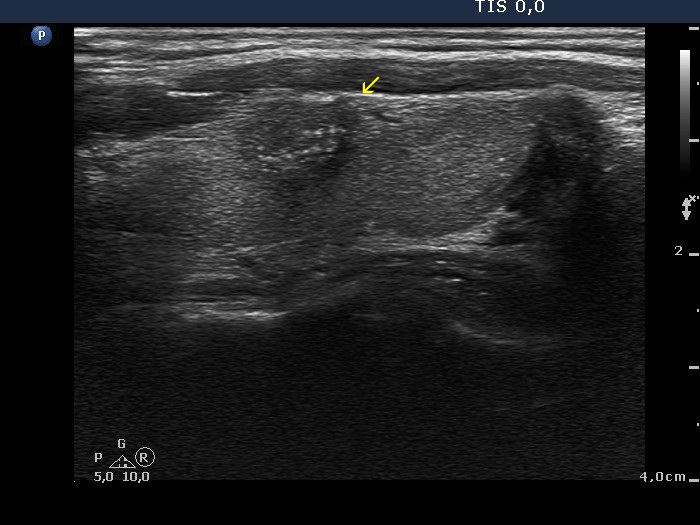
Papillary carcinoma (histology) - case conp032 |
|
Transverse scan |
Longitudinal scan |
 |
 |
 |
 |
|
|
Benign nodular goiter (cytology) - case 2117 |
Papillary carcinoma (cytology) - case 2057 |
 |
 |
 |
 |
|
|
Benign nodular goiter (cytology) - case 2054 |
Benign nodular goiter (cytology) - case 2056 |
 |
 |
 |
 |
|
|
Benign nodular goiter (cytology) - case 2024 |
Benign nodular goiter (cytology) - case 2140 |
 |
 |
 |
 |
|
|
Benign nodular goiter (cytology) - case 2107 |
Benign nodular goiter (cytology) - case 2109 |
 |
 |
 |
 |
|
|
Hashimoto's thyroiditis (cytology) - case 1496 |
Benign nodular goiter (cytology) - case 2050 |
 |
 |
 |
 |
|
|
Hashimoto's thyroiditis (cytology) - case 1768 |
Hashimoto's thyroiditis (cytology) - case 2168 |
 |
 |
 |
 |
|
|
Hashimoto's thyroiditis (cytology) - case 2168 |
|
 |
 |
|
|
Hashimoto's thyroiditis (cytology) - case 430 |
Benign nodular goiter (cytology) - case 2109 |
 |
 |
 |
 |
|
|
|
|
Hashimoto's thyroiditis (cytology) - case 880 |
Benign colloid goiter (cytology) - case 2120 |
 |
 |
 |
 |
|
|
|
|
Hashimoto's thyroiditis (cytology) - case 479 |
Benign hyperplastic nodules and Hashimoto's thyroiditis (histology) - case 54 |
 |
 |
 |
 |
|
|
Hashimoto's thyroiditis (cytology) - case 2080 |
Papillary carcinoma (cytology) - case 2057 |
 |
|
 |
|
|
|
|
|
Subacute, de Quervain's thyroiditis (cytology) - case 1454 |
|
 |
 |
|
|
Papillary carcinoma and Hashimoto's thyroiditis (histology) - case 2138 |
|
Papillary carcinoma and Hashimoto's thyroiditis in the right lobe |
Hashimoto's thyroiditis in the left lobe |
 |
 |
 |
 |
|
|