Table 2. Non-pathological causes of lobulated margins |
||
The essence of pathological lobulation is that it occurs at the external surface of a single nodule and is caused by the nodule. So, external and not internal border, the surface of a single nodule and not the surface of a mass composed of multiple nodules, and pathological nodule and not discrete lesion of Hashimoto's thyroiditis.
The cause of a pathological lobulation is the infiltrative growth of the nodule, the ultrasound sign of which is the undulation on the nodule' border. The similar phenomenon, undulation on the margin can be caused by other reasons. This might be the basic anatomy, which should be follow the thyroid and the nodule within the thyroid. Another issue arises in the event of thyroiditis when the primary infiltrative process is the thyroiditis which invades the nodule. In resected thyroids, scars and adhesions make the surface of the thyroid or a recurrent nodule within a lobe undulated. There is another form of non-pathological lobulation which can be seen in cysts after aspiration of the fluid; the initially regular borders occasionally get lobulated.
The greatest concern is the distinction between solitary and multinodular goiters in a large composite mass. This issue cannot be always resolved. We start with examples of this problem.
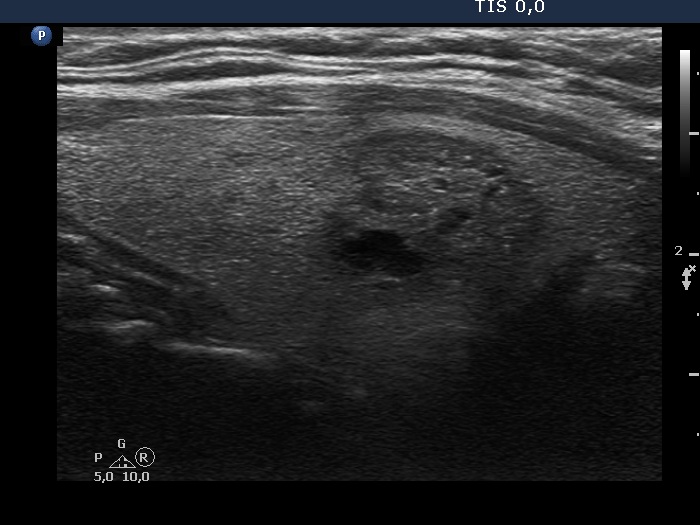
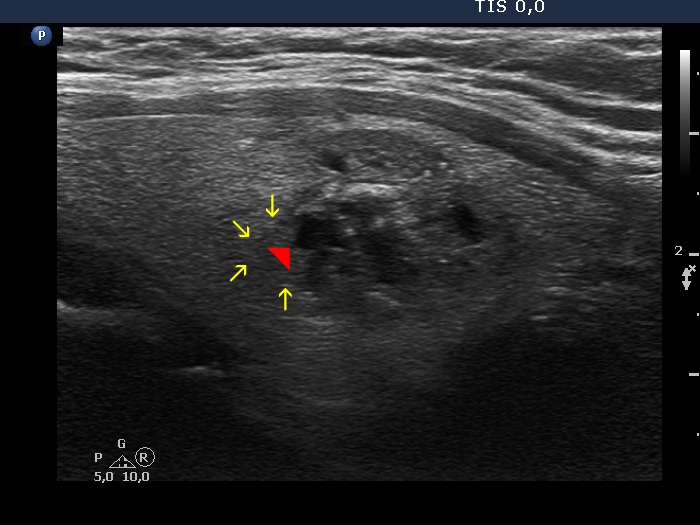
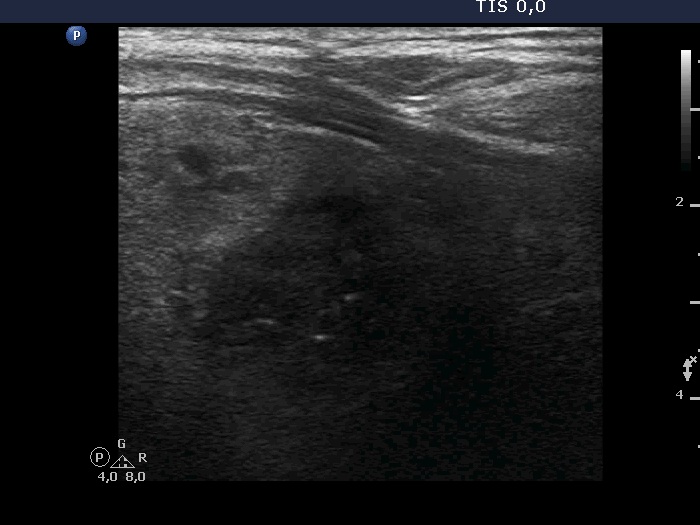
Papillary carcinoma (histology) - case conp042 |
|||||||
Transverse scan |
Longitudinal scan |
||||||
 |
 |
||||||
|
|||||||
Benign nodular goiter (cytology) - case 2024 |
|||||||
Transverse scan |
Longitudinal scan |
||||||
 |
 |
||||||
|
|||||||
Benign nodular goiter (cytology) - case 2116 |
|||||||
Transverse scan |
|||||||
 |
 |
||||||
Longitudinal scan |
|||||||
 |
 |
||||||
|
|||||||
Benign nodular goiter (cytology) - case 2115 |
|||||||
 |
 |
||||||
 |
 |
||||||
|
|||||||
Benign nodular goiter (cytology) - case 2054 |
|||||||
Transverse scan |
Longitudinal scan |
||||||
 |
 |
||||||
 |
 |
||||||
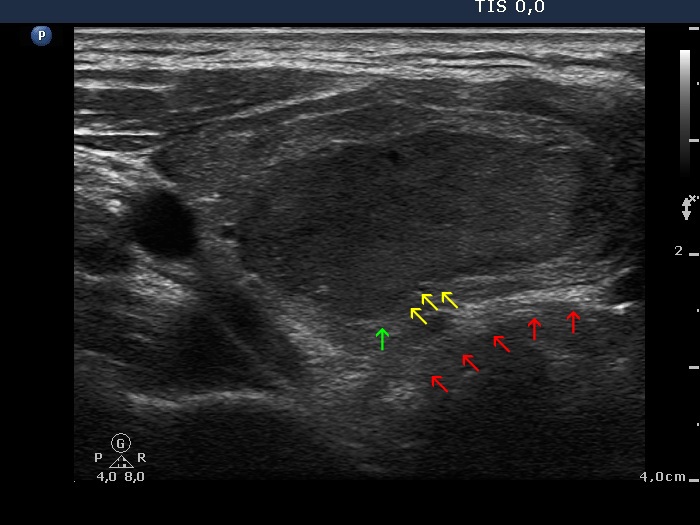
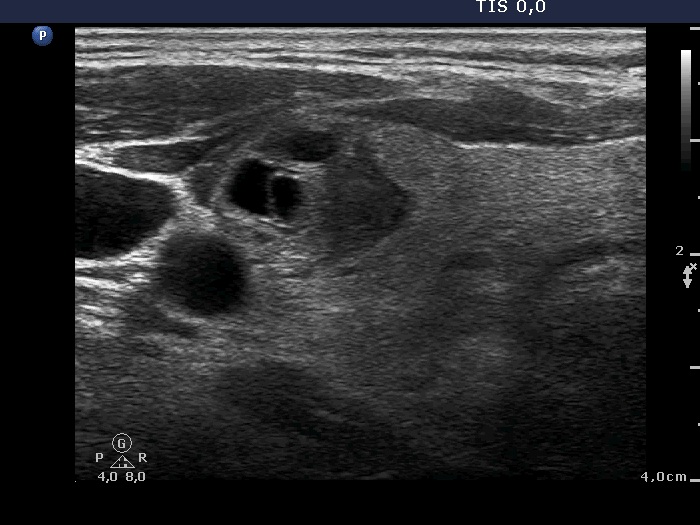
The issue is again the presence of multiple nodules: the entire nodular area seems to have lobulated margins, but in fact this is not a solitary nodule having lobulated margins but a cluster of smaller discrete lesions. |
|||||||
Benign nodular goiter (cytology) - case 2054 |
|||||||
|
 |
||||||
|
|||||||
Benign nodular goiter (cytology) - case 2157 |
|||||||
Transverse scan |
Longitudinal scan |
||||||
 |
 |
||||||
 |
 |
||||||
|
|||||||
Benign nodular goiter (cytology) - case 2018 |
|||||||
Transverse scan |
Longitudinal scan |
||||||
 |
 |
||||||
|
|||||||
Follicular adenoma in patient with Graves' disease (histology) - case 408 |
|||||||
Transverse scans |
|||||||
 |
 |
||||||
|
|||||||
|
|||||||
|
|||||||
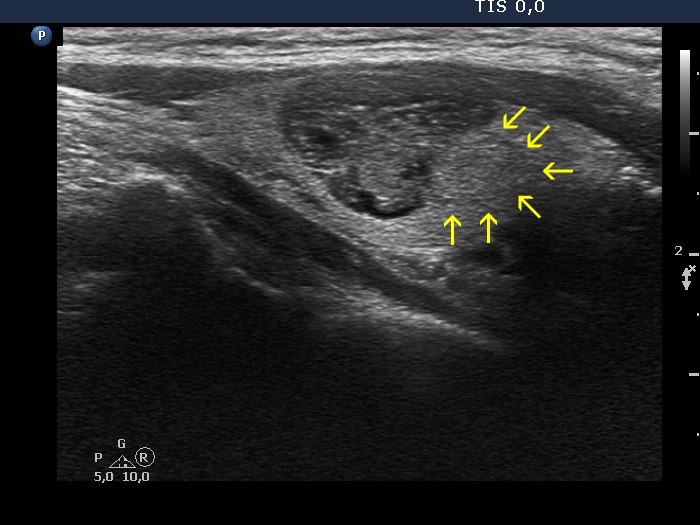
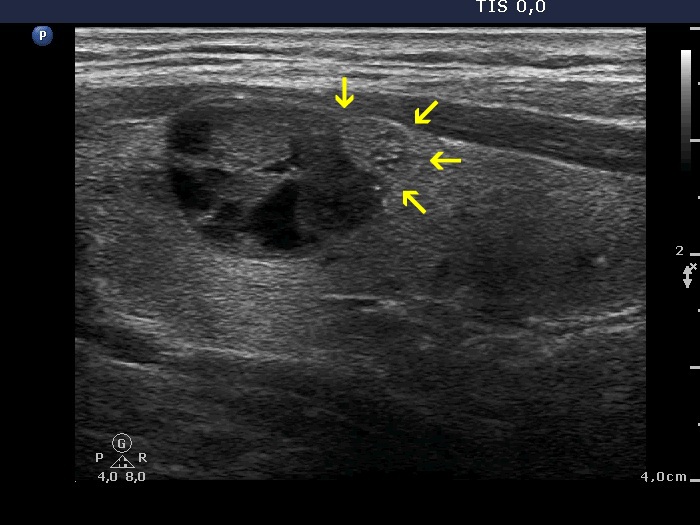
| Note that the projection (yellow arrows) of the cyst toward the isthmic part of the thyroid can be recognized even at the 4-year follow up when the nodule became significantly smaller. This projection simply followed the anatomical situation before the treatment and this distortion remained permanent. This projection should not be judged as a sign of abnormal, pathological border. We must be aware of the possibility of such pattern in nodules has been treated either with ethanol or laser of radiofrequency or in cyst which has been diminished with simple aspiration: the original distorted shape remains unchanged. | |||||||
Benign, colloid goiter (cytology) - case 2152 |
|||||||
Transverse scan |
Longitudinal scan |
||||||
 |
 |
||||||
 |
 |
||||||
|
|||||||
Benign, colloid goiter (cytology) - case 186 |
|||||||
Transverse scan |
Longitudinal scan |
||||||
 |
 |
||||||
 |
 |
||||||
|
|||||||
Recurrent hyperthyroidism after an insufficient surgery (clinical diagnosis) - case 17 |
|||||||
Transverse scans (upper the right, lower the left lobe) |
Longitudinal scans (upper the right, lower the left lobe) |
||||||
 |
 |
||||||
 |
 |
||||||
|
|||||||
A patient with benign cyst - case 2062 |
|||||||
Before the aspiration |
After the aspiration |
||||||
 |
 |
||||||
 |
 |
||||||
|
|||||||
A patient with benign cyst - case 1275 |
|||||||
Before the aspiration |
After the aspiration of 14 mL cystic fluid |
||||||
 |
 |
||||||
 |
 |
||||||
|
|||||||


