Table 8. The issue of thyroiditis |
||
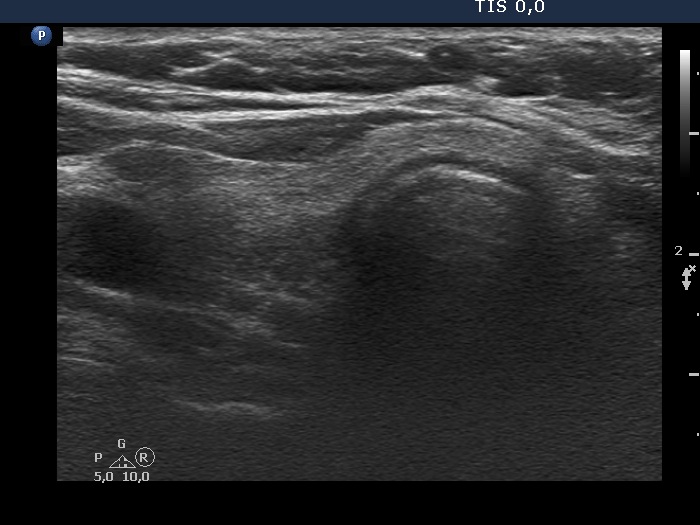
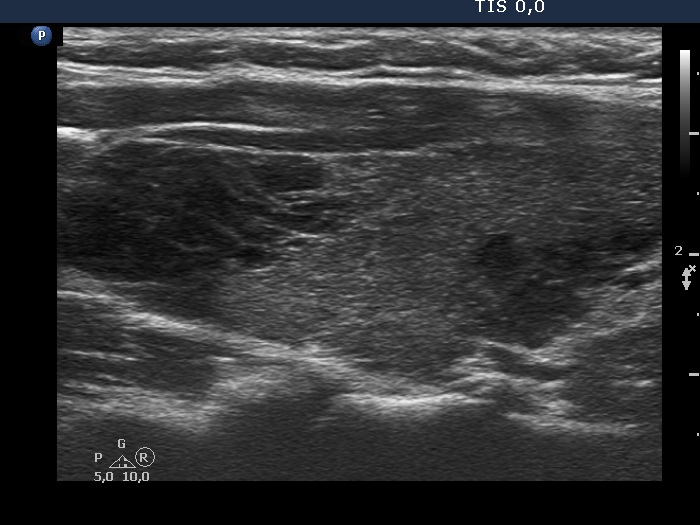
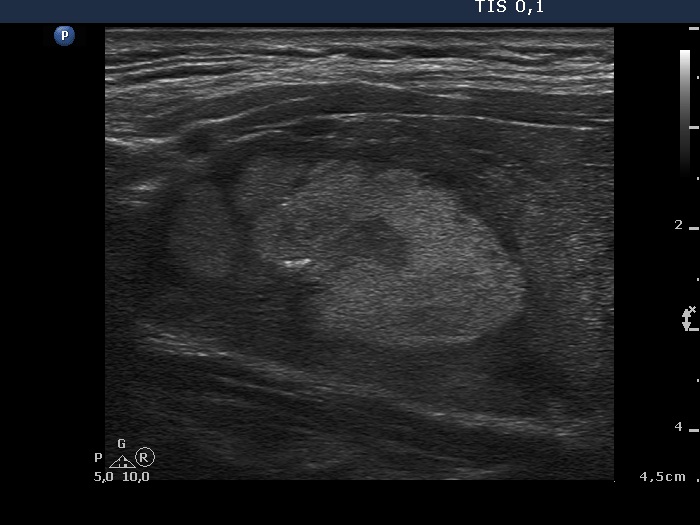
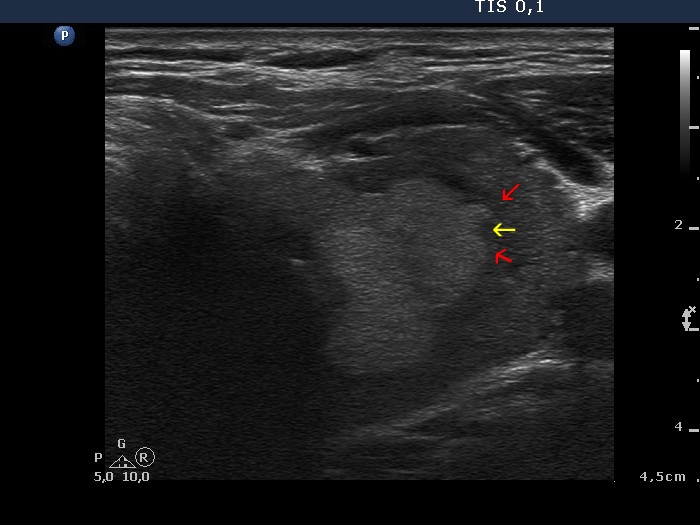
Both Hashimoto's and de Quervain's thyroiditis cause differential diagnostic issue in the judgement of nodule borders. The former is characterized by discrete hypoechoic lesions in more than 90% of cases. These discrete areas usually have blurred or puzzle-like, spiculated margins. The issue is not the presence of abnormal borders but the presence of pathological nodule. We face with another problem in the coexistence of Hashimoto's thyroiditis and pathological nodules. The underlying thyroiditis can infiltrate the nodule and makes the appearance of the nodule lobulated. Therefore, in most of these cases the primary event is the infiltrative process of the thyroiditis, and not that of the nodule. It means that these irregularities of nodule borders should not be encountered among irregular borders.
Both types of thyroiditis frequently present blur of the discrete areas.
Hashimoto's thyroiditis - case 2108 |
|
 |
 |
|
|
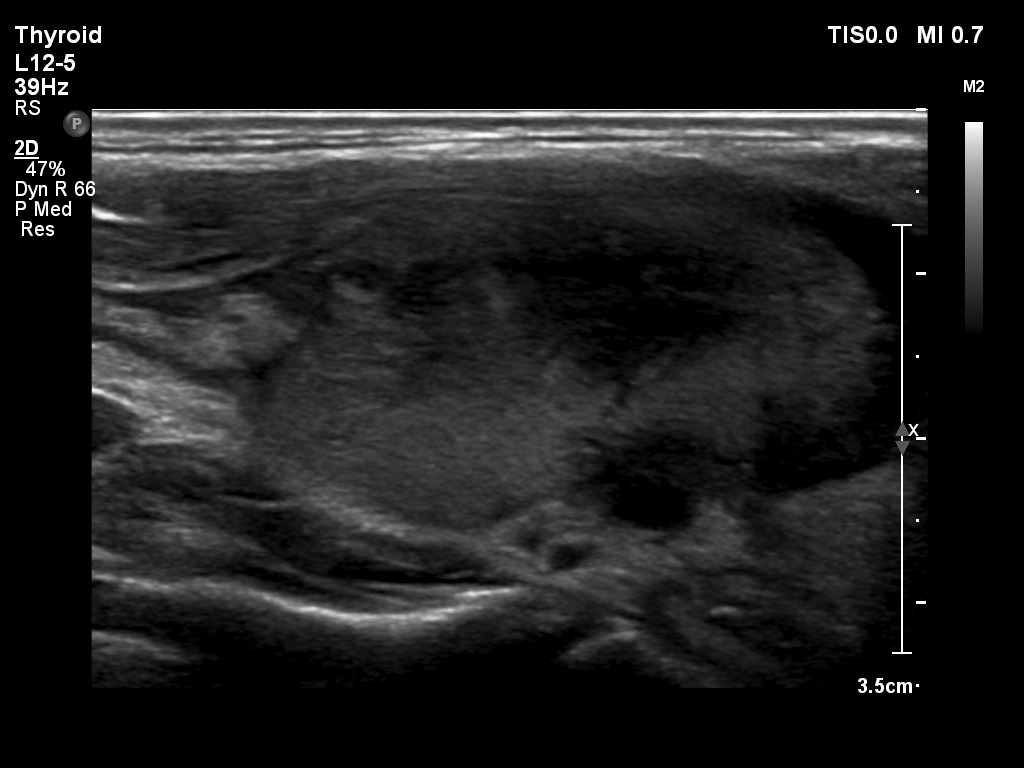
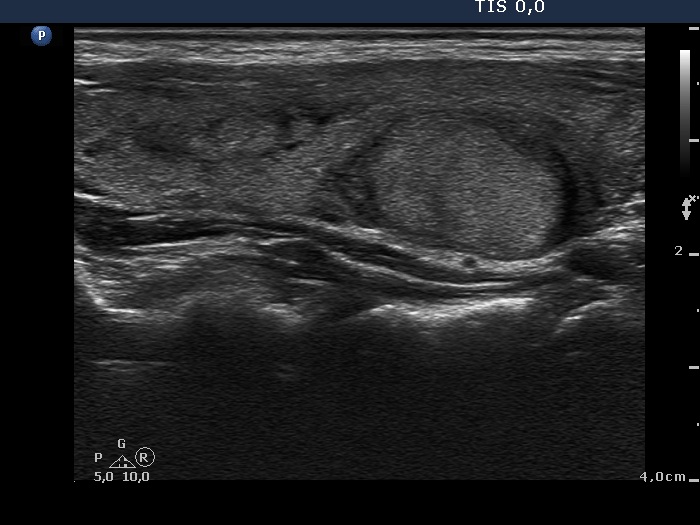
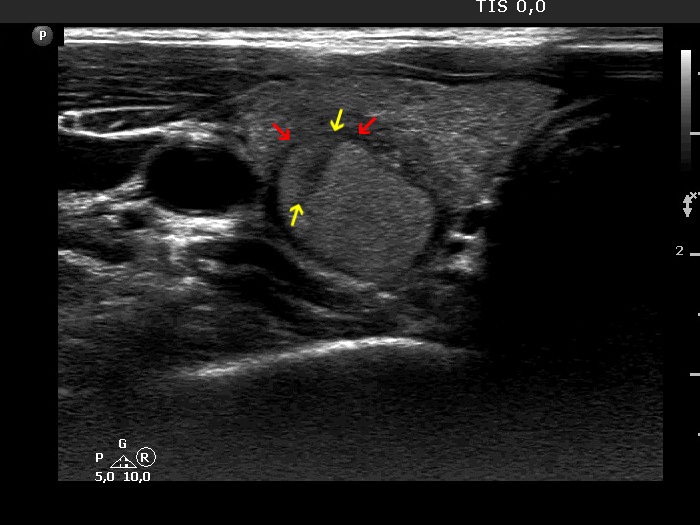
Subacute, de Quervain's thyroiditis (cytology) - case 1036 |
Subacute, de Quervain's thyroiditis (cytology) - case 1454 |
 |
 |
 |
 |
|
|
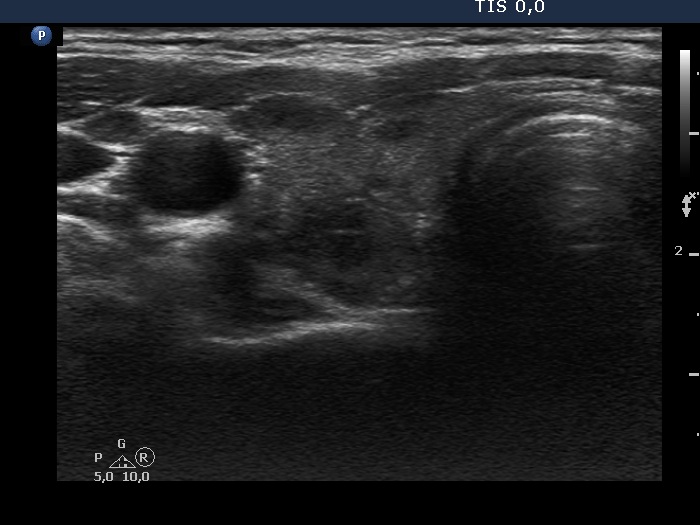
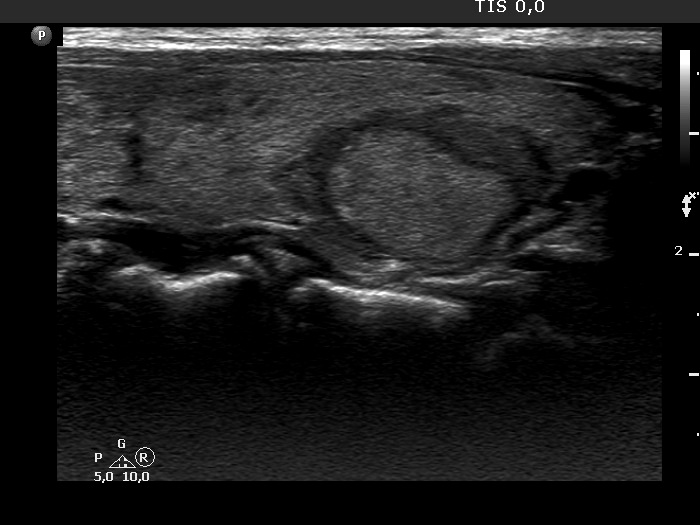
Hashimoto's thyroiditis (cytology) - case 1188 |
|
Transverse scans |
Longitudinal scans |
 |
 |
 |
 |
|
|
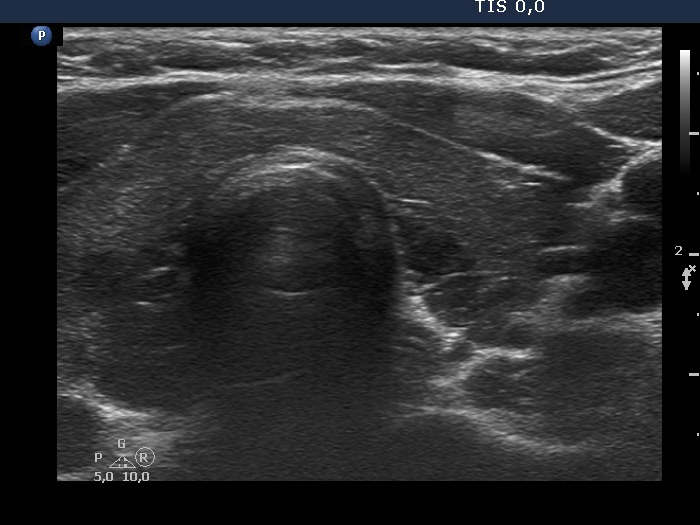
Hashimoto's thyroiditis (cytology) - case 430 |
|
Transverse scan |
Longitudinal scan |
 |
 |
|
|
Hashimoto's thyroiditis (cytology) - case 2080 |
Hashimoto's thyroiditis (cytology) - case 1496 |
 |
 |
 |
 |
|
|
Hashimoto's thyroiditis (cytology) - case 2168 |
|
 |
 |
 |
 |
|
|
Hashimoto's thyroiditis (cytology) - case 54 |
|
 |
 |
 |
 |
|
|