|
 |
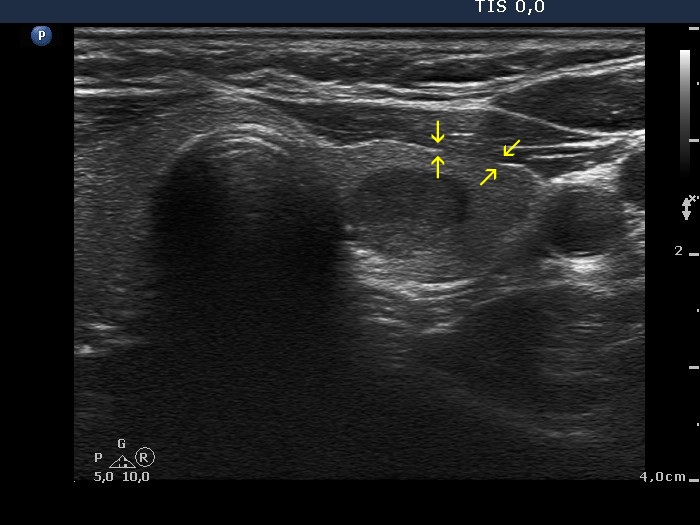 |
The echogenic line running on the ventral surface of the thyroid is lacking between the two pairs of arrows. In this case this phenomenon cannot be caused by extrathyroidal spread.
|
| |
|
|
Transverse scan |
Longitudinal scan |
 |
 |
The nodule' contour is abutting at the dorsal part. The abutment exceeds 25%. The capsule is all along continuous at this part of lobe. Note that the thyroid capsule in the ventral surface is discontinuous which has no relevance because here the nodule is not abutting.
|
| |
Benign hyperplastic nodule (histology) - case 2050 |
 |
 |
The capsule is discontinuous not only in those parts where the nodule presents abutment. (Red arrowheads point to the capsule of the lobe, while yellow arrows do to those parts where the capsule is lacking.)
|
| |
|
Sclerotherapy of a benign cystic nodule - case 2068 |
Before the second session of sclerotherapy |
Four years after the sclerotherapy |
 |
 |
 |
 |
Initially the nodule presented non-abutting contour because there was a thin echonormal parenchyma between the ventral surface of the nodule and the thyroid. At the follow-up, the contour became abutting. The capsule was non-visible at the first, while became discontinuous at the follow-up examination.
|
| |
|
|
Transverse scan |
Longitudinal scan |
 |
 |
 |
 |
The hyperechogenic line on the ventral surface of the lobe is all along intact in the transverse scan, while the more complex echogenic structure seen in the longitudinal scan is not broken.
|
| |
|
A patient after aspiration of a benign cyst - case 2062 |
Before the aspiration |
After the aspiration |
 |
 |
 |
 |
At first sight, the pattern seems to be suspicious of extrathyroidal spread. In the upper right image, the origin of the ventral wing-like hypoechogenic structure is equivocal. Considering the left upper image, the run of the extrathyroidal strap muscle is more evident. The dorsal wall of the strap muscle is marked with yellow arrows. Nevertheless, the ventral wall of the hypoechogenic nodule is in direct contact with the muscle fiber.
|
The cyst before the aspiration
|
 |
|
 |
 |
For an experienced investigator, this pattern should not cause any concern regarding extrathyroidal spread. The only area which might theoretically raise the possibility of extrathyroidal spread is only a technical artifact: be aware the we can follow an acoustic artifact (marked with red) up to the most ventral part of the image.
On the other hand, this case meets all criteria on which extrathyroidal spread should be considered: protrusion of the nodule into the adjacent tissue, capsular bulging and disruption (green arrows). The definition fails in the event of dominantly cystic nodules.
|
| |
|
 |
 |
The medial part of the nodule was difficult to judge, partly because of the focus was set improperly (red arrow), partly because of the acoustic shadow caused by the cartilage. The improper setting of the focus also contributed to the difficulty of proper judgement of the borders at its the dorsomedial part (yellow arrow).
|
| |
|
|
 |
 |
 |
 |
The arrows point to those parts of the lobe where the capsule has been broken. Nonetheless, in this case the thyroid capsule was almost continuous at the medial part.
|
|
|