Selected topics - differentiation of discrete lesions - Table 4. Intralesional echogenic figures in Hashimoto's thyroiditis |
||
There is one echogenic figure which significantly more often occurs in autoimmune thyroiditis; this is connective tissue. The hallmark of this echogenic figure is the synchronous presence of echogenic lines and granules. We cannot overemphasize the importance of the correct ultrasound analysis. One of the most frequent failures in thyroid ultrasound is the misinterpretation of connective tissue as microcalcification.
All other echogenic figures occur significantly less frequently in Hashimoto's thyroiditis than in thyroid nodules. Moreover, the presence of coarse calcifica t ion or microcalcification is a strong argument against that a discrete lesion would be a hypoechogenic area in Hashimoto's thyroiditis. The presence of microcalcification is the most important ultrasound feature to recognize a papillary cancer focus among similarly hypoechogenic areas of Hashimoto's thyroiditis.
Hashimoto's thyroiditis - case 1652 |
|
 |
 |
The hypoechogenic areas present both echogenic lines and granules which synchronous presence is the hallmark of connective tissue. Note the multiplicity, the irregular shape and borders of these lesions. All of these properties stand for these lesions being presentations of Hashimoto's thyroiditis. |
|
Hashimoto's thyroiditis - case 1268 |
|
Right lobe, horizontal scan |
Right lobe, longitudinal scan |
 |
 |
|
|
Benign hyperplastic nodule in a Graves' patient (histology) - case 1673 |
|
 |
 |
The presence of coarse calcification is a strong argument that the lesion is a true nodule. |
|
Papillary carcinoma in Graves' disease - case 993 |
|
Right lobe, horizontal view |
Right lobe, longitudinal view |
 |
 |
There are several bright punctate echogenic foci and less bright granules and lines, as well. The former corresponds to microcalcifications, while the latter does to connective tissue. |
|
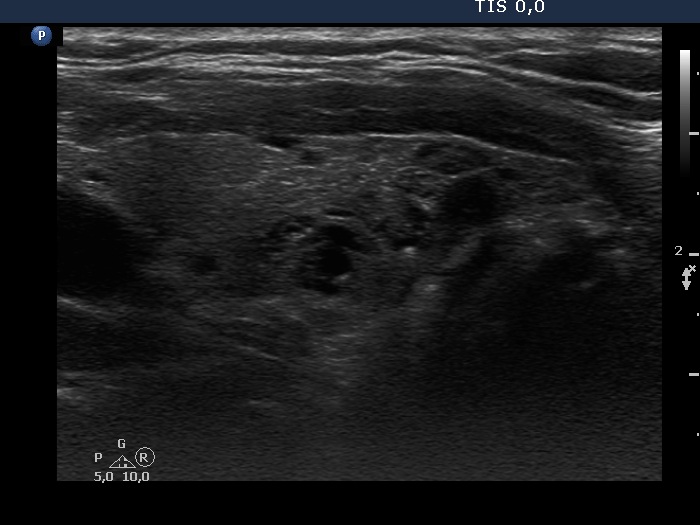
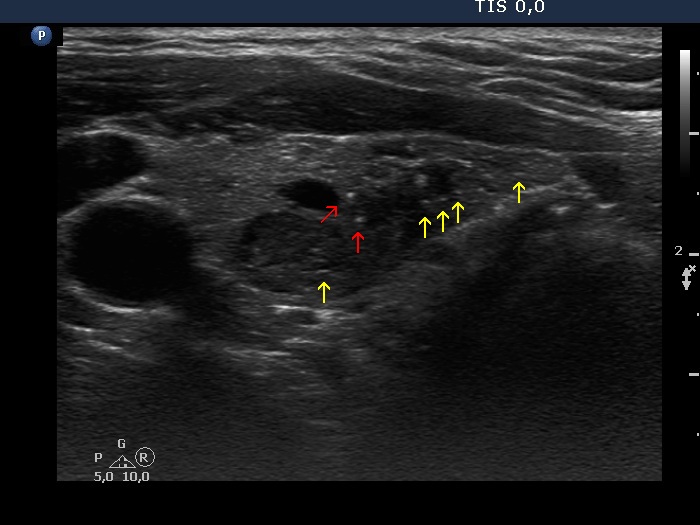
Hashimoto's thyroiditis - case 1617 |
|
Right lobe, horizontal scan |
Right lobe, longitudinal scan |
 |
 |
 |
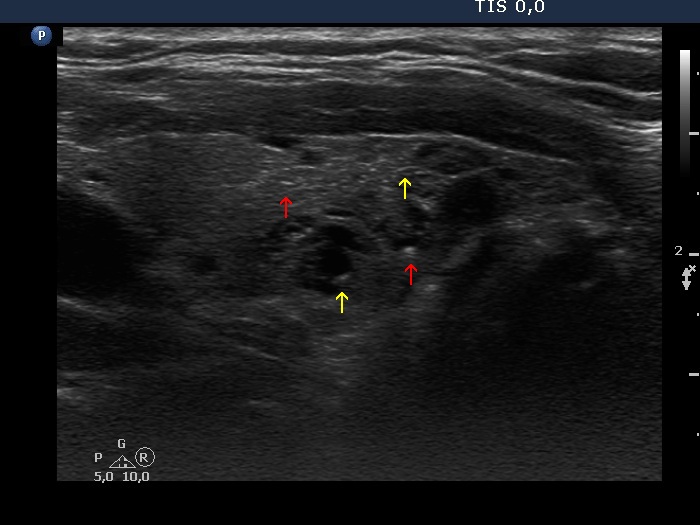 |
The interpretation of smaller and less bright granules and lines (yellow arrows) is not very difficult, they correspond to connective tissue. On the other hand, there are a few more bright and a bit larger echogenic granules (red arrows). The finding of one similarly bright line in the right image is of help: these figures are also very likely presentations of connective tissue. |
|
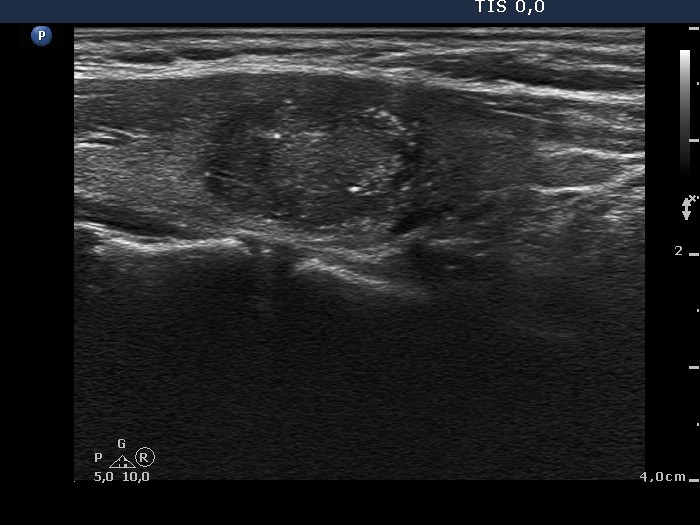
Hashimoto's thyroiditis - case 1048 |
|
Right lobe, horizontal scans |
Right lobe, longitudinal scans |
 |
 |
 |
 |
|
|
Papillary carcinoma in Graves' disease - case conp035 |
|
First examination |
Follow-up 18 months later |
 |
 |
 |
 |
|
|
Graves' disease without any nodules - case 888 |
Papillary carcinoma in Hashimoto's thyroiditis - case conp009 |
 |
 |
 |
 |
|
|
|
|
Hashimoto's thyroiditis (histology) - case 441 |
Papillary carcinoma in Hashimoto's thyroiditis - case conp061 |
 |
 |
 |
 |
|
|
|
|
Papillary carcinoma in Hashimoto's thyroiditis - case 1589 |
|
Right lobe, horizontal scan |
Right lobe, longitudinal scan |
 |
 |
The thyroid is composed of discrete hypoechogenic areas. The tumor focus presents punctate echogenic foci, as well. |
|
Papillary carcinoma in Hashimoto's thyroiditis - case conp057 |
|
Right lobe, horizontal scan |
Right lobe, longitudinal scan |
 |
 |
|
|
Papillary carcinoma in Hashimoto's thyroiditis - case conp016 |
Hashimoto's thyroiditis - case 389 |
 |
 |
 |
 |
|
|
Hashimoto's thyroiditis and suspicion of papillary carcinoma (histology in progress) - case 1483 |
|
Right lobe |
Left lobe |
 |
 |
 |
 |
|
|