
|
|
The composition of the nodule - case 956
|
|

Clinical presentation: A 46-year-old woman was referred for aspiration of a nodule discovered on evaluation of diffuse complaints suggesting thyroid dysfunction.
Palpation: no abnormality.
Result of blood test: TSH 0.55 mIU/L.
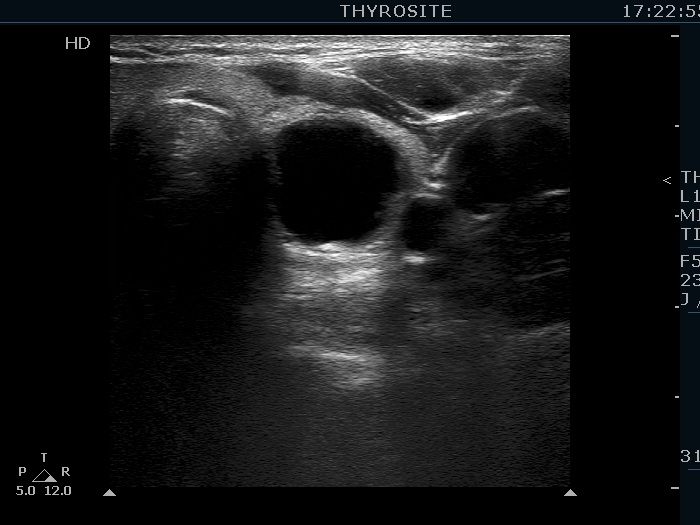
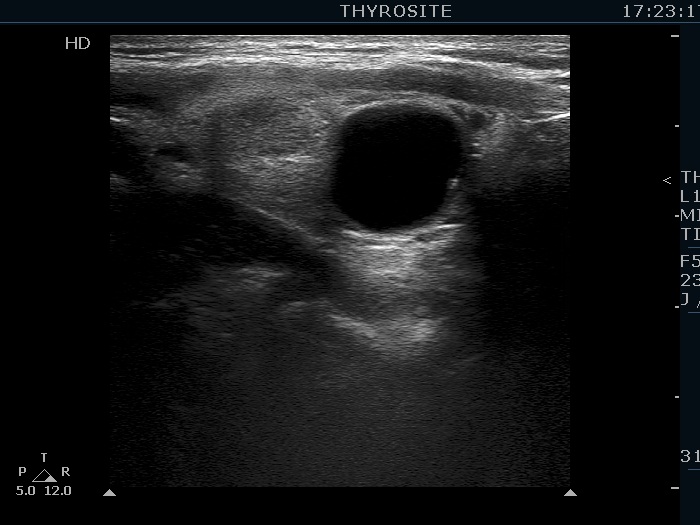
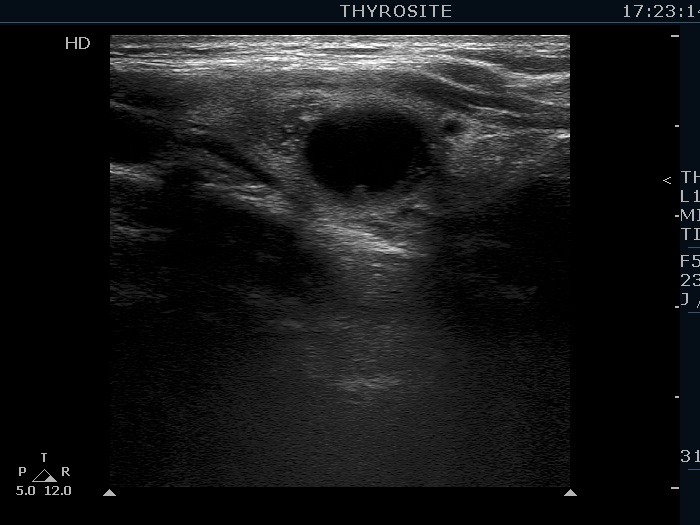
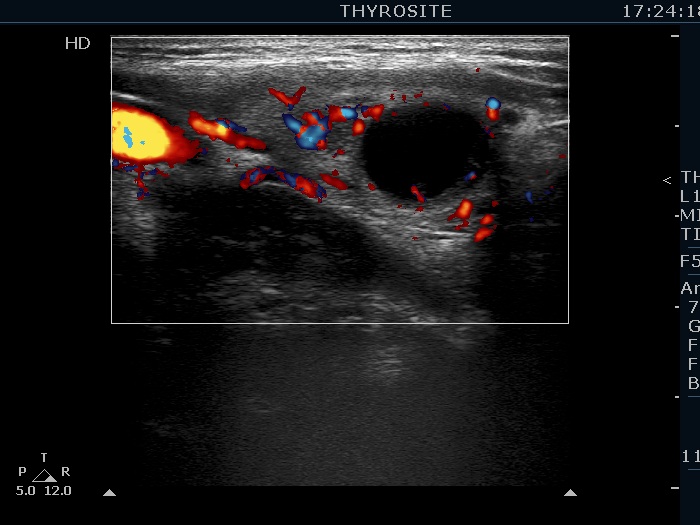
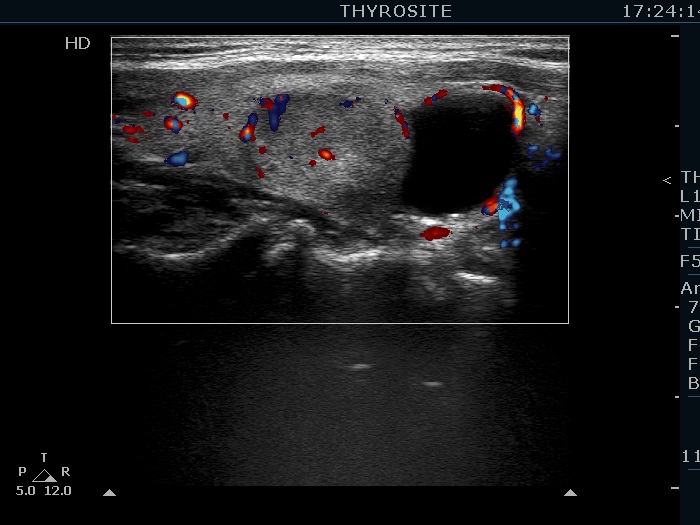
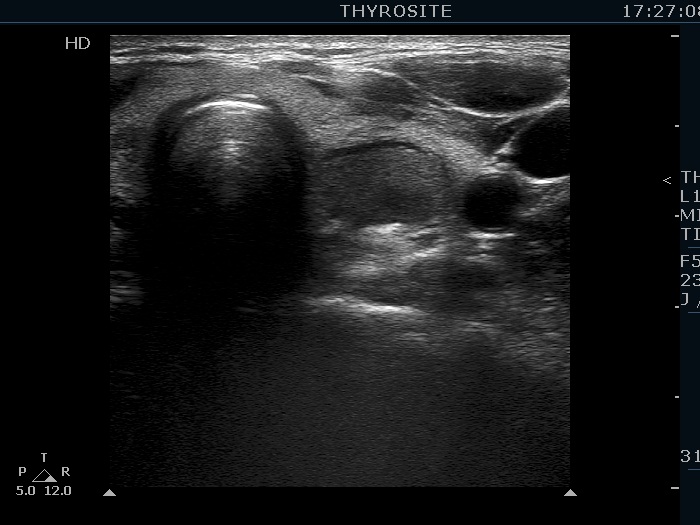
Ultrasonography. The thyroid was echonormal. There were several hypoechogenic lesions in the right lobe. The left lobe had an upper, solid and a lower cystic nodule. The former had both echonormal and moderately hypoechogenic parts and presented halo sign. The cystic nodule had a very tiny solid area in the dorsal part. Nonetheless, before aspiration it was unclear whether this would be a pure cyst or not. After aspirating 2 mL serous fluid a large, moderately hypoechogenic solid area replaced the previous cystic field and it became evident that this is in fact a central type cystic nodule.
Aspiration cytology of both nodules resulted in benign report.
Comment. This case illustrates why is it unsubstantiated to diagnose a pure cyst before aspiration. First, even the existence of a pure thyroid cystic nodule is debated if we use the term 'nodule' in pathological sense. Great proportion of smaller pure cystic lesions are in fact dilated macrofollicles covered with only few layers of follicular cells. Such cystic lesions completely disappear after the removal of the cystic content. But these lesions are not true nodules. Secondly, in most cases of true cystic nodules, which seem to be a pure cyst before aspiration, a solid area will appear after the removal of cystic content.