
|
|
Subacute granulomatous thyroiditis - case 363
|
|


















Initial examination (1st and 2nd rows of images):
Clinical presentation: A 45-year-old woman requested evaluation because of right-sided neck sensitivity which started a few weeks ago. Her thyroid was already examined 12 years ago. She was then euthyroid and the aTPO value was 344. Then an annual check was recommended.
Palpation: The right lobe was tender on palpation.
Laboratory examination: TSH 1.67 mIU/L, anti-TPO 0.5 U/mL, CRP 3.40 mg/L (normal value below 5).
Ultrasonography: There thyroid was echonormal. There were multiple hypoechoic lesions in the right lobe. These had irregular and blurred borders. The left lobe was almost intact.
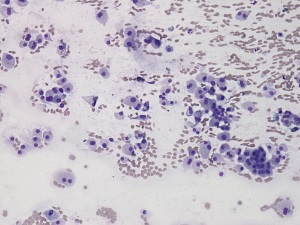
FNA was performed. There were almost exclusively oxyphilic cells on the smear. No lymphoid elements were found. The pattern corresponded to an oxyphilic tumor.
Considering the clinical presentation, we gave a common clinical-ultrasound-cytological diagnosis of oxyphilic cell proliferation which is probably part of thyroiditis.
Suggestion. Non-steroid anti-inflammatory drug was administered. We recommended a repeat ultrasound in 3 months.
Examination 4 weeks later (3rd row of images):
Clinical presentation: The patient's complaints intensified significantly. The right side of the neck became painful and the left side became sensitive.
Palpation: The right lobe was spontaneously painful, while the left lobe was tender. Both lobes were hard.
Laboratory tests: TSH 2.66 mIU/L, FT4 12.6 pM/L, CRP 10.5 mg/L.
Ultrasonography: Although the extent of hypoechoic areas in the right lobe were unchanged, the lobe significantly increased in size. Hypoechoic areas have appeared in the left lobe.
Suggestion. Take methylprednisolone for 6 weeks, starting with 32 mg a day and then in gradually decreasing doses. Repeat examination in 6 to 12 weeks.
Examination 2 years later (4th row of images):
Clinical presentation: The patient's complaints ceased within 24 hours and did not recur.
Palpation: no abnormality.
Laboratory tests: TSH 3.30 mIU/L, anti-TPO 0,6 U/mL.
Ultrasonography: The right lobe was echonormal or minimally hypoechoic. No deeply hypoechoic lesions of pathological importance were found.
Suggestion. Yearly TSH test.
Comments.
-
Perhaps the most important lesson of the case is that, in justified cases, it is not only possible to deviate from the guidelines, but occasionally we must deviate from the recommendations. We do not have a 100% reliability test in medicine. This cytological picture alone would have warranted surgery as it corresponded in all respects to a Hürthle cell tumor. Taking the clinical and ultrasound presentation into account was the pivotal to avoid unnecessary surgery.
-
Most likely, this patient has an underlying autoimmune thyroiditis. This is backed both by the elevated aTPO years before the first examination, and the ultrasound pattern at the last visit. The patient indisputably had a clinically subacute thyroiditis. The lack of elevated aTPO stands against a subacute lymphocytic thyroiditis while the elevated CRP level favors a subacute granulomatous form.
-
Most textbooks notice that de Quervain's thyroiditis is characterized by the presence of non-metaplastic follicular cells. Obviously, this is true for most cases. However, granulomatous thyroiditis arising in Hashimoto's thyroiditis, is the exception, as demonstrated in this patient.