
|
|
Teamwork - case 2540
|
|




Clinical presentation: A 61-year-old woman requested a second opinion. She was operated on 16 years ago when a subtotal resection of the left lobe was performed. Histopathology disclosed benign, hyperplastic nodules. A few months ago, she noticed in the mirror that her thyroid gland was enlarged. On evaluation in another hospital, the nodule was described as a TIRADS 4 category nodule and cytology resulted in a Bethesda III, follicular lesion of unknown significance. The endocrinologist told the patient, that surgery will probably be needed.
Palpation: There was a not firm nodule in the right side of the isthmus.
Result of blood test: TSH 1.53 mIU/L.
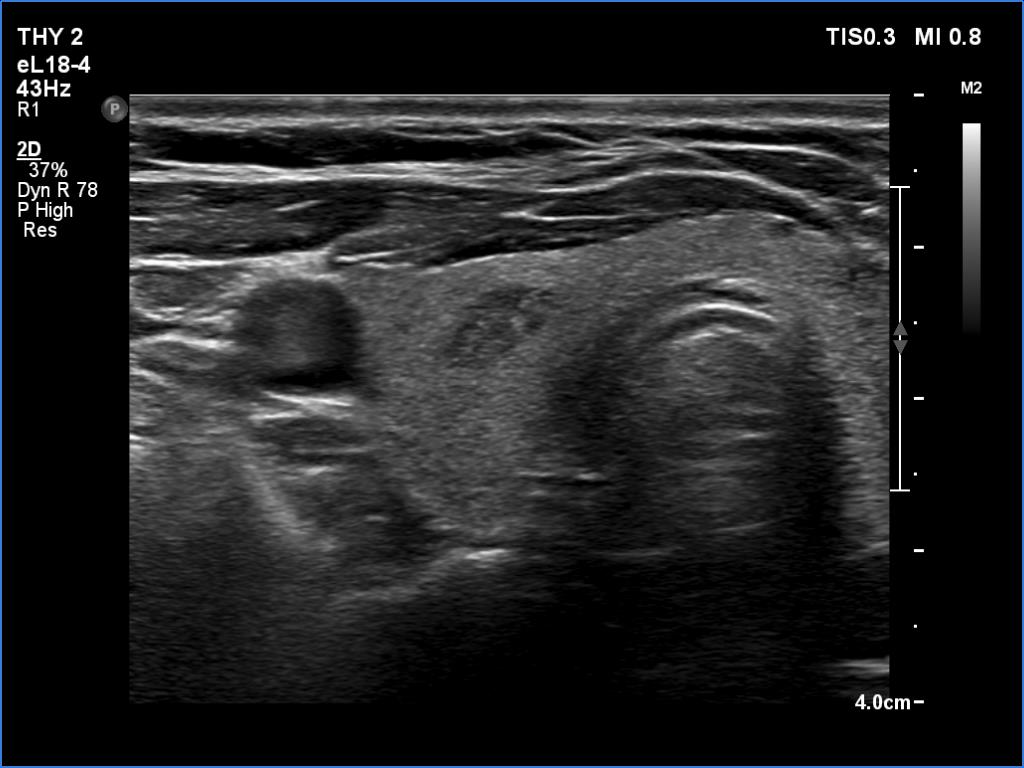
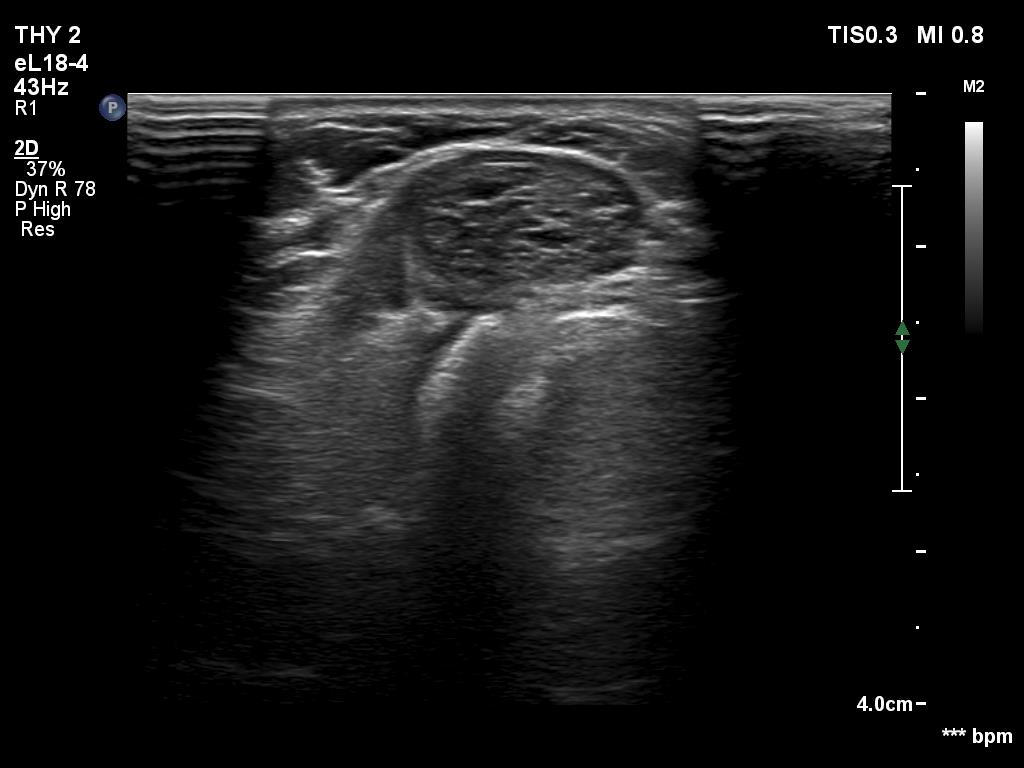
Ultrasonography. The thyroid was echonormal. There were several minimally hypoechoic discrete lesions in both lobes. Corresponding to the palpable nodule, a mixed, solid-cystic nodule was found which had spongiform areas. The solid part was minimally/moderately hypoechoic. The lesion did not show halo and presented neither intranodular nor perinodular blood flow.
Suggestion. I told the patient that based on the ultrasound pattern of the nodule, the risk of malignancy was extremely low. I suggested that unless it bothers her aesthetically, it is not worth having surgery. A repeat ultrasound was advised in a year.
Comments.
-
Although the nodule belongs indeed to TIRADS 4 lesions, the risk of malignancy is practically zero in nodules with such presentation. This is probably an evolving spongiform cyst. A significant proportion of solid area has been already disappeared.
-
The risk of follicular cancer can be excluded. Follicular cancer is only exceptionally cystic and almost always presents either halo sign or perinodular blood flow.
-
The usual straightforward approach suggested by the protocols can occasionally lead to wrong decisions. The only chance to avoid surgery in such cases is the evaluation of all available data including the reconsideration of ultrasound.