
|
|
Teamwork - case 699
|
|







Clinical presentation: A 25-yr-old woman was referred for a repeat evaluation. She was diagnosed with a nodular goiter. Cytology of the right nodule resulted in benign colloid goiter while the result of FNA was follicular neoplasia in the event of the left lesion. Considering the small size of the latter, the endocrinologist requested a second opinion.
Palpation: There was a moderately firm nodule in the right lobe.
Laboratory tests: euthyroidism.
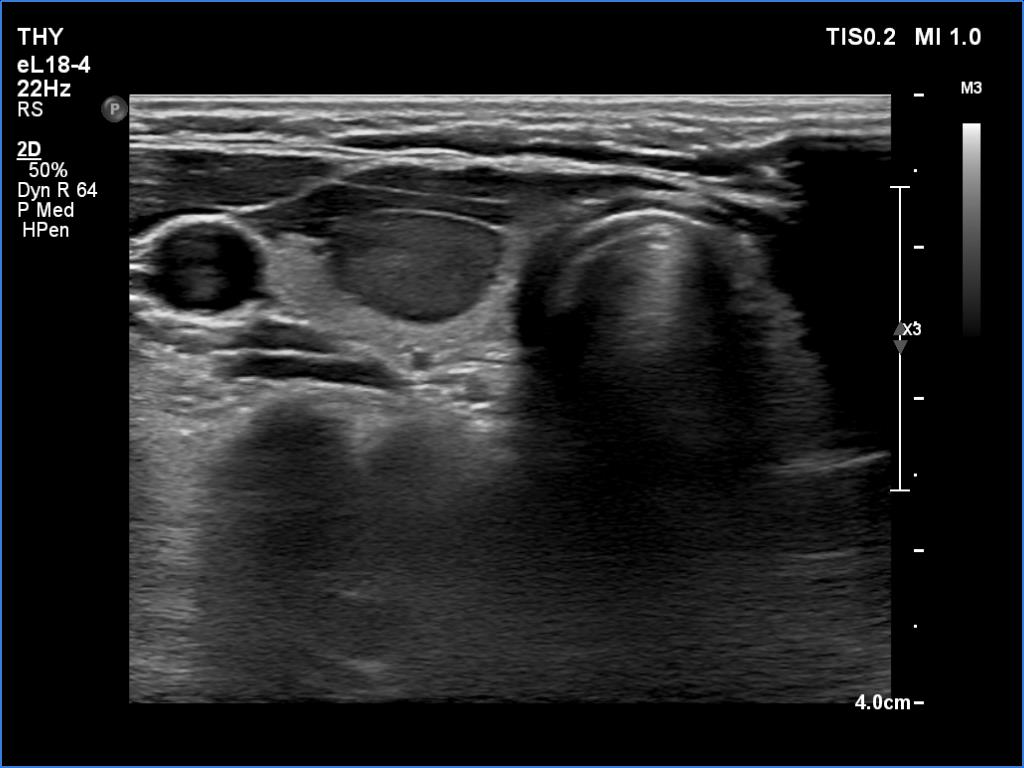
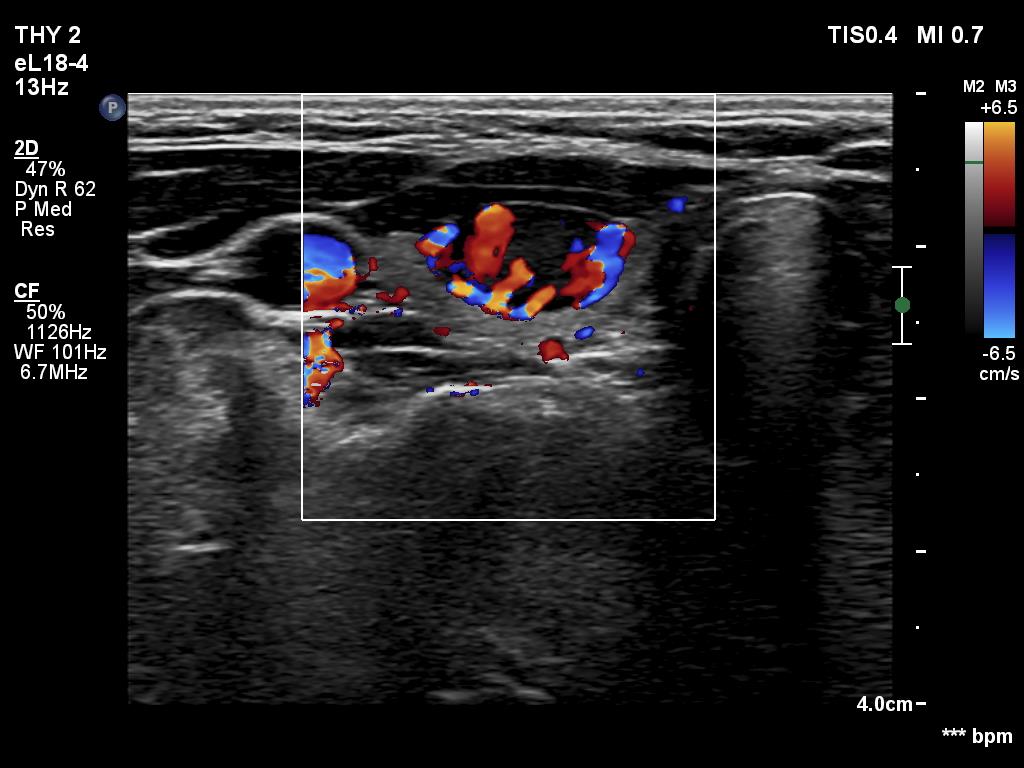
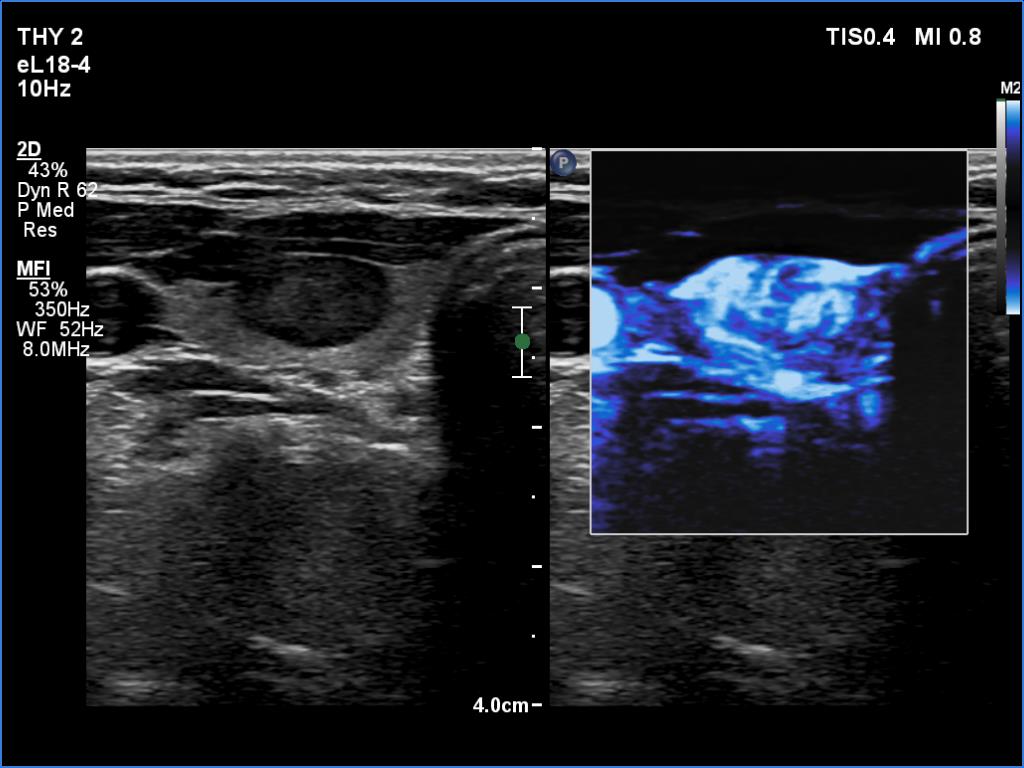
Ultrasonography. The thyroid was echonormal. There was a moderately hypoechoic nodule in the ventral part of the right lobe. This lesion has regular, sharp margins and presented signs of a possible extrathyroidal spread. The intranodular vascularity was increased. The left lobe had a tiny, minimally hypoechoic lesion. The largest diameter was 7 mm. The lesion had both echogenic lines and granules, a pattern corresponding either to connective tissue or back wall figure. The lesion had neither halo nor perinodular blood flow.
We performed FNA from both lesions. Considering the ultrasound image, it could not be ruled out that the previous examiner might have exchanged the smear. In both cases, cytology resulted in benign colloid goiter.
Suggestion: ultrasound in a year.
Comment.
-
The nodule in the right lobe is remarkable because of the hypoechogenicity, the increased vascularity and because it shows sing of a possible extrathyroidal spread.
-
The case study reveals several issues.
-
The original sin was the misinterpretation of connective tissue as microcalcification.
-
The second problem is whether to indicate an FNA in a subcentimeter suspicious nodule. None of the TIRADS take a clear position. While the main table of these systems does not recommend sampling for such nodules, each protocol makes cytology a consideration in the text.
-
The third was the handling of the cytology. This was not the failure of the colleagues but the failure of our current practice. If we follow the suggestions, we cannot take clinical or ultrasound data into account when giving a cytological diagnosis. It is very strange because in the histopathological diagnosis, these data are taken into account. Moreover, while in histopathology, the consideration of these data only rarely influences the final diagnosis, in cytology, this consideration would have a huge impact. Regarding this case, a nodule which does not show any ultrasound signs of a capsule, is unlikely a follicular tumor; this lesion did not have either a halo sign or perinodular blood flow.
-
We should never forget that the basic unit of the thyroid is the follicle, and even non-nodular thyroid can present with microfollicular proliferation. Considering the fact that every fifth to every third cytologically diagnosed follicular neoplasia proves to be non-tumorous lesion, the consideration of clinical and particularly ultrasound data is very helpful. The negligence of these data inevitably leads to unnecessary surgeries.
-