
|
|
Case 115
|
|







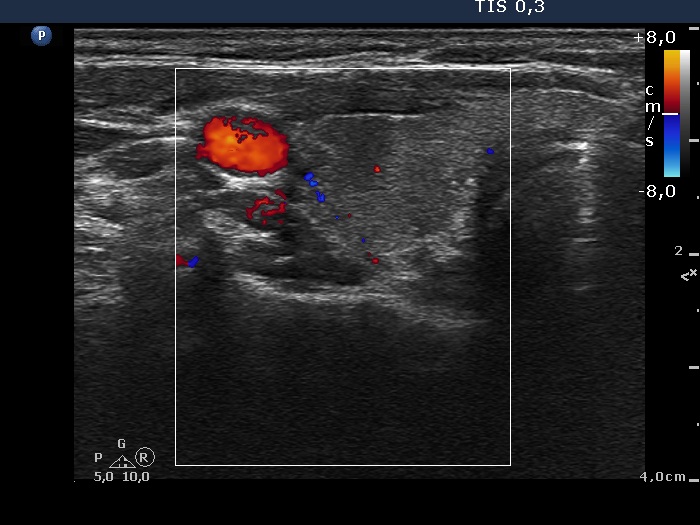





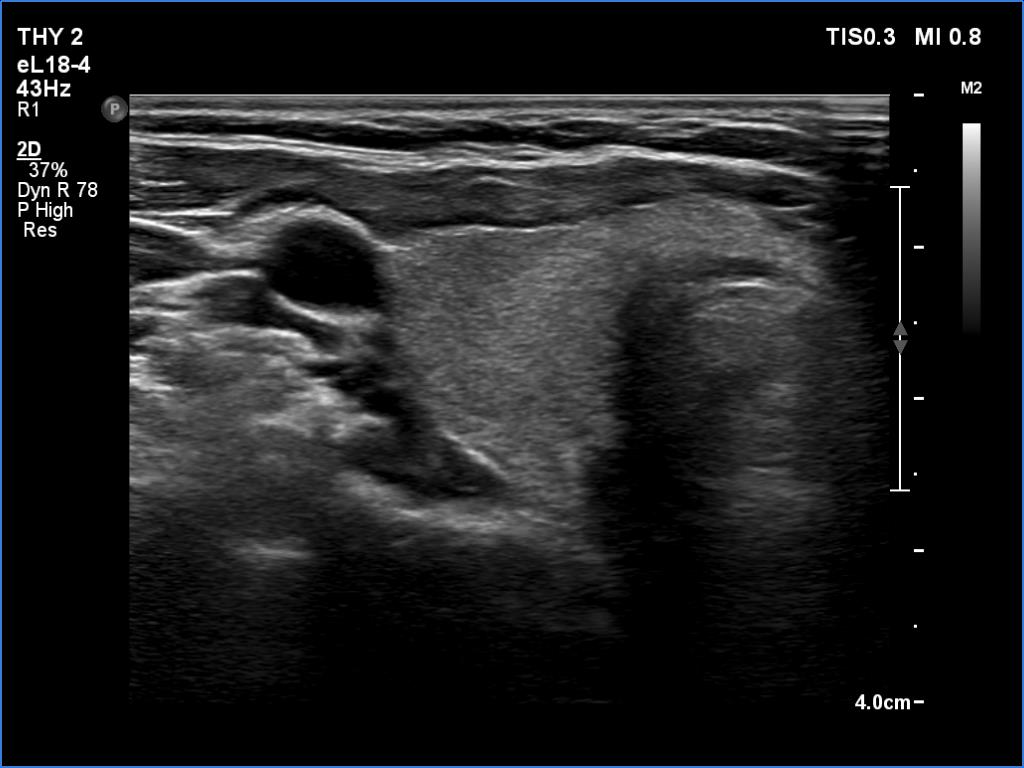
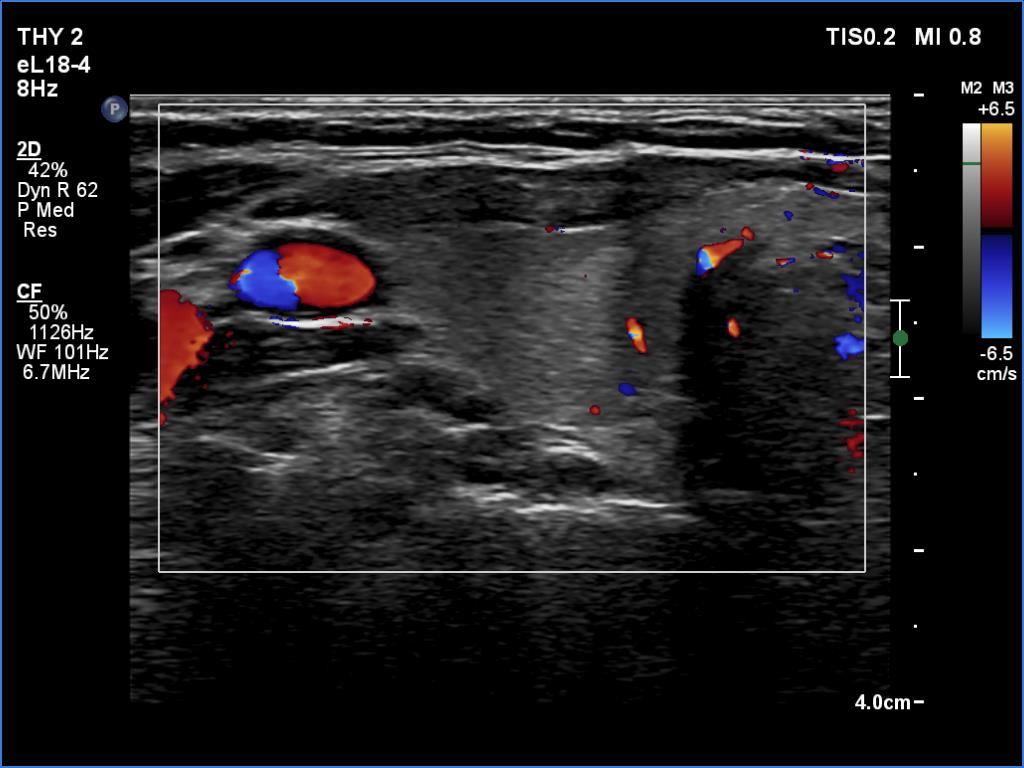


Initial examination (first row of images):
Clinical presentation: A 39-year-old woman was referred for evaluation of neck complaints lasting for more than a month. The patient had fever, neck pain. She has got two courses of antibiotics and non-steroid anti inflammatory drugs which had no effect.
Palpation: The right lobe was painful and hard while the left lobe was tender.
Laboratory examination: TSH 0.01 mIU/L, FT4 29.1 pM/L, FT3 7.45 pM/L, CRP 31.2 mg/L.
Ultrasonography: The thyroid presented with hypoechoic areas which had blurred borders. The echogenicity index was approximately 65% in the right and 20% in the left lobe. The thyroid was almost completely avascular.
Diagnosis: subacute, granulomatous de Quervain's thyroiditis.
Suggestion. Steroid therapy was suggested.
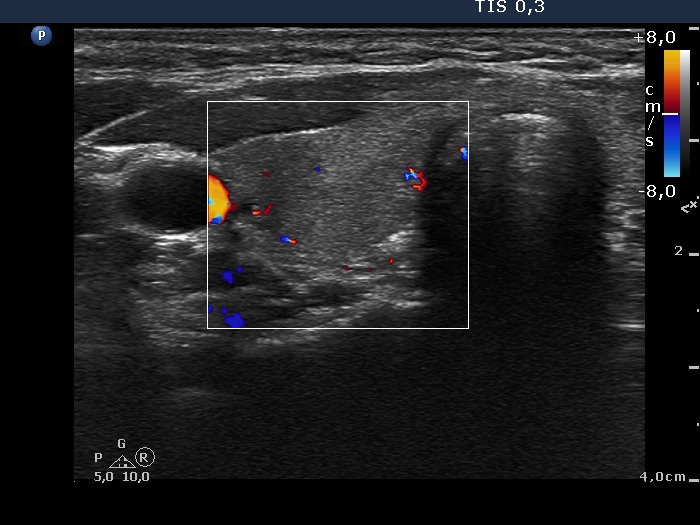
Follow-up 2 months after the first visit (3rd row of images):
Clinical presentation: Within 24 hours of the administration of 32 mg methylprednisolone, the neck complaints and subfebrility had stopped. When the patient reduced the dose to 8 mg daily for 2 weeks as suggested, the left lobe became sensitive. This tenderness has now been significantly reduced, but still persisted at times.
Palpation: The left lobe was tender on palpation.
Laboratory tests: TSH 1.62 mIU/L, FT4 9.97 pM/L, CRP 0.1 mg/L.
Ultrasonography: The right lobe decreased in size as did the extent of hypoechogenic areas in this lobe. The left lobe remained unchanged.
Suggestion: Discontinuation of steroid therapy. TSH in three months.
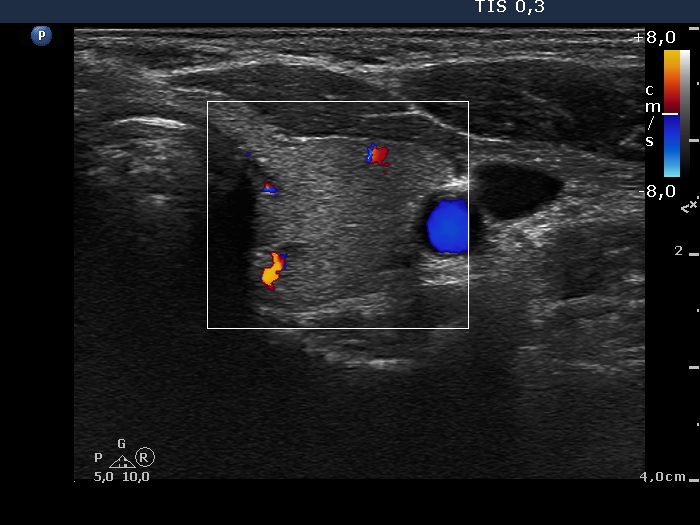
Follow-up 6 months after the first visit (3rd row of images):
Clinical presentation: The patient had no complaints.
Palpation: no abnormality.
Laboratory tests: TSH 2.06 mIU/L, FT4 13.3 pM/L, CRP 0.3 mg/L.
Ultrasonography: The pattern of the entire thyroid became almost completely normal. Only small hypoechoic areas were observed.
Suggestion: TSH in six months, in the event of pregnancy at once.
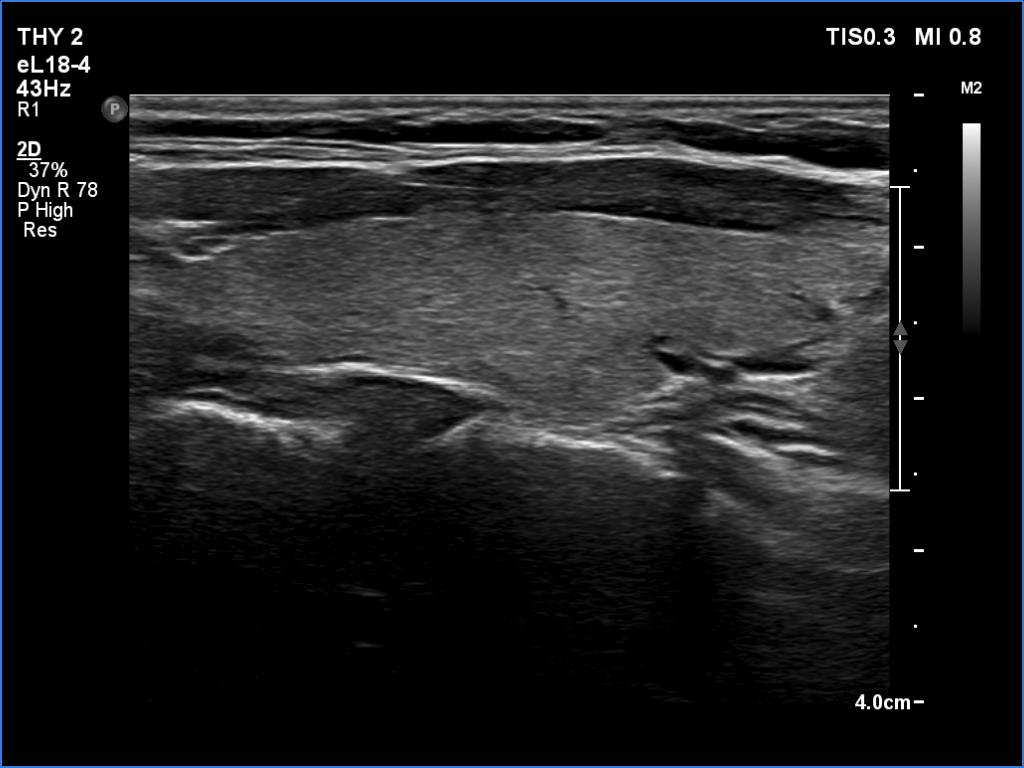
Follow-up 5 years later (3rd row of images):
Clinical presentation: Six months after the previous visit the patient became pregnant. The TSH was 5.91 mIU/L at the 5th gestational weeks. Replacement therapy was given which was ceased after delivery. The patient was free of complaints and the TSH was in the normal range, even during a next pregnancy 2 years later. Recently, a few weeks after COVID-19 infection, she noticed tenderness in the right side of the neck.
Palpation: no abnormality.
Laboratory tests: TSH 1.72 mIU/L, CRP 3.5 mg/L.
Ultrasonography: The thyroid was intact.
Comment.
-
This is one of the characteristic courses of subacute thyroiditis.
-
We always suggest TSH evaluation if the patient becomes pregnant within 5 years after a granulomatous, subacute thyroiditis.
- A discrete hypoechoic lesion of thyroiditis frequently resembles a suspicious nodule with blurred and lobulated margins and nonparallel orientation, as happened in this case. We must be aware of the clinical data when analyzing an ultrasound pattern.