
|
|
Case 1764
|
|










First examination (first row of images):
Clinical presentation. A 26-year-old woman requested an evaluation because of complaints suggesting hyperthyroidism. She lost 3 kg in weight, had fatigue and nervousness. She had been treated for Graves' disease for one year, the thyrostatic was stopped 10 months ago.
Palpation: no abnormality.
Laboratory examination: TSH 0.91 mIU/L, FT4 13.4 pM/L.
Ultrasonography. The thyroid was echonormal and presented several hypoechogenic areas. The echogenicity index was < 10%. The vascularization was average or a bit decreased.
Suggestion: to continue follow-up, hormonal evaluation in a year, in the event of complaints suggesting relapse of hyperthyroidism or pregnancy at once. We advised to visit a gastroenterologist.
Follow-up examination 8 months after the previous visit (second row of images):
Clinical presentation. The previous symptoms were resolved after administering antacids. Four weeks prior to the present examination the patient noticed an increased heart rate and other complaints suggesting relapse of the hyperthyroidism. In contrast with the first episode of Graves' disease, thyroid associated ophthalmopathy has appeared.
Palpation: unchanged.
Laboratory examination: TSH 0.001 mIU/L, FT4 43.1 pM/L.
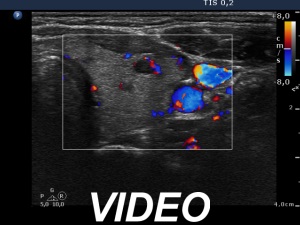
Ultrasonography. The thyroid became more hypoechogenic, the echogenicity index has increased to 50% as had the vascularization. Multiple hypoechogenic areas have appeared, none of them fit to a nodule in a pathological sense.
Suggestion: daily 20 mg methimazole and surgery after restoration of FT4-level.
A total thyroidectomy was performed. Histopathology disclosed diffuse goiter and focal lymphocytic thyroiditis.