
|
|
Case 861
|
|


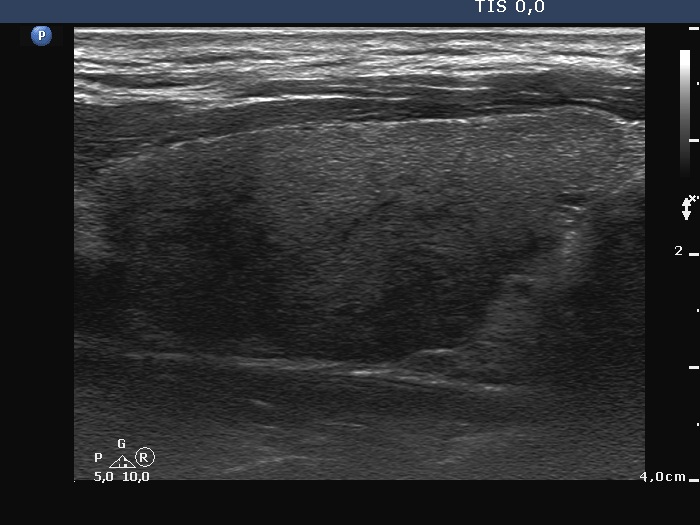





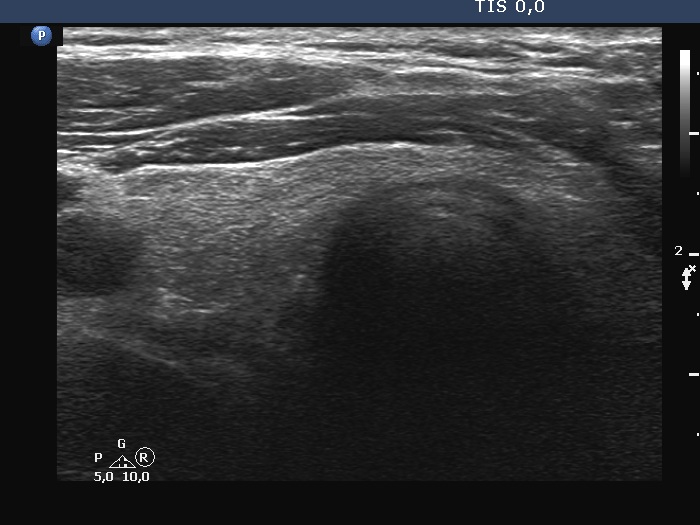



Initial examination (first row of images):
Clinical presentation: A 43-year-old man was referred for evaluation of neck complaints which have started 6 weeks ago when both sides of the neck became tender and occasionally painful. The patient noticed recurrent fever. Non-steroid anti-inflammatory drugs had only temporary effect.
Palpation: Both lobes were hard and painful on palpation.
Laboratory examination: TSH 0.02 mIU/L, FT4 28.7 pM/L, aTPO < 28 U/mL, CRP 55.7 mg/L
Ultrasonography: Both lobes had hypoechoic areas which showed ill-defined borders. The echogenicity index was around 50%. The hypoechoic areas were avascular.
Suggestion. Six-week steroid therapy.
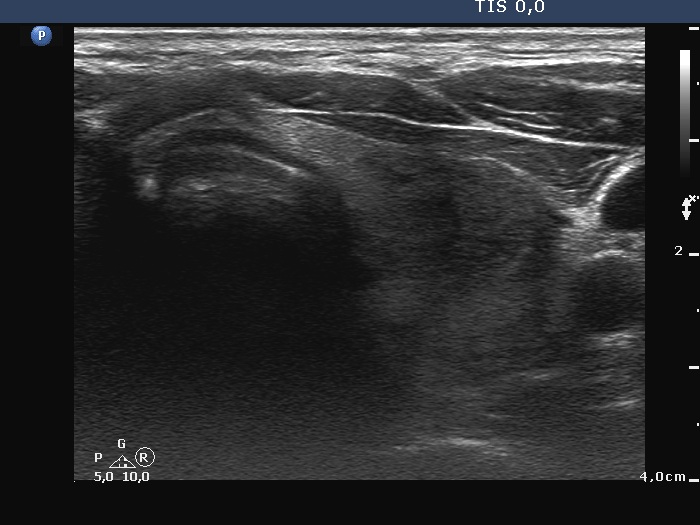
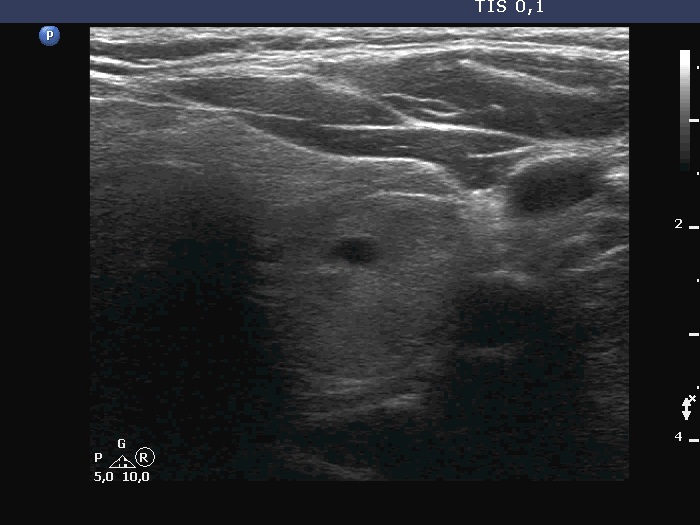
Examination 7 months later (second row of images):
Clinical presentation: The patient became asymptomatic within 12 hours after the first dose of methyl-prednisone and remained so.
Palpation: no abnormality.
Laboratory tests: TSH 1.03 mIU/L, FT4 14.2 pM/L, CRP 0.7 mg/L.
Ultrasonography: Both the size of the nodule and the extent of hypoechoic areas have decreased. An isoechoic nodule has appeared which was obscured by hypoechogenicity in the previous study. The vascularity was still very scanty.
Suggestion. Follow-up in 2 years.
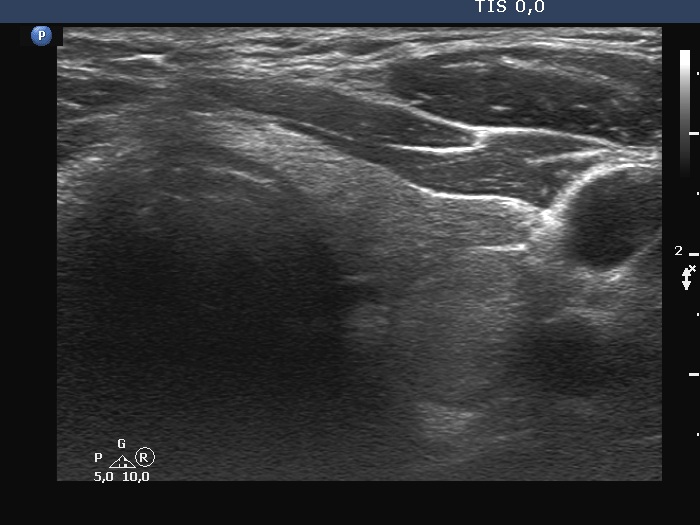
Examination a year after the first visit (third row of images):
Clinical presentation: The patient had no complaints.
Palpation: no abnormality.
Laboratory tests: TSH 1.60 mIU/L, FT4 15.6 pM/L, aTPO 12 U/mL.
Ultrasonography: The dorsal part of the right lobe remained hypoechoic. The nodule in the left lobe has increased in size and presented halo and signs of perinodular vascularity.
Cytology of the nodule resulted in benign lesion.
Suggestion: repeat examination in three years.
Comment. In the active phase of subacute thyroiditis, a nodule can be obscured. The real structure of the thyroid can be revealed only when the hypoechogenicity disappears or decreases significantly.