
|
|
100 consecutive cases of papillary cancer - case 093
|
|









Clinical presentation: A 61-year-old man was referred for evaluation with a suspicion of a metastatic thyroid cancer. The patient noticed a large, tender mass in the right side of the neck 3 weeks ago. On evaluation, multiple suspicious lymph nodes were diagnosed in the right side of the neck while both thyroid lobes were described as having suspicious nodules. The patient has got two courses of antibiotics and noticed a decrease in the neck mass in the five days which elapsed after the initiation of FNA.
Palpation: Both lobes had a firm nodule. There was a soft 4 cm large mass several centimeters above the thyroid while another, smaller, very firm node was palpated above the right lobe. The right lobe was tender while neither the lymph nodes nor the left lobe was tender.
Functional state: TSH 0.48 mIU/L, CRP 17.2 mg/L, aTPO 21 U/mL.
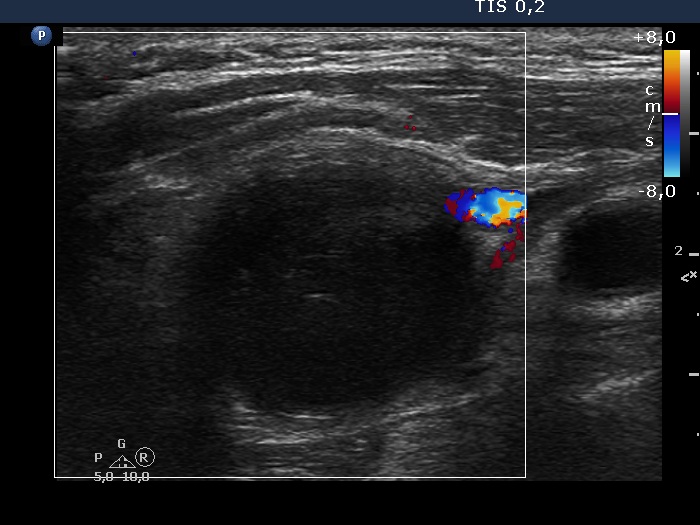
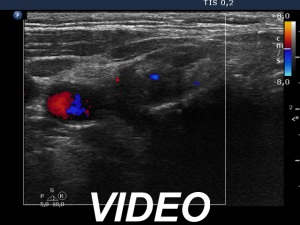
Ultrasonography. The thyroid was echonormal and had numerous tiny hypoechoic areas. There was a deeply hypoechoic lesion in the right lobe. This lesion had irregular, spiculated margins. There was a moderately hypoechoic nodule in the left lobe. This nodule had microcalcifications and showed both taller-than-wide and taller-than-long shape.
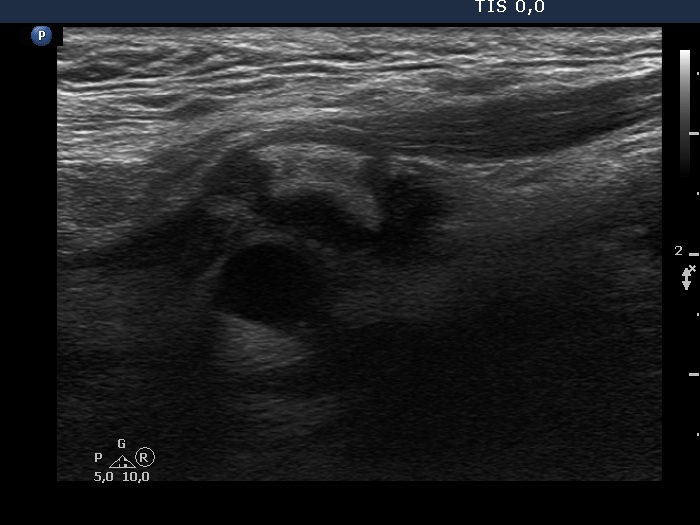
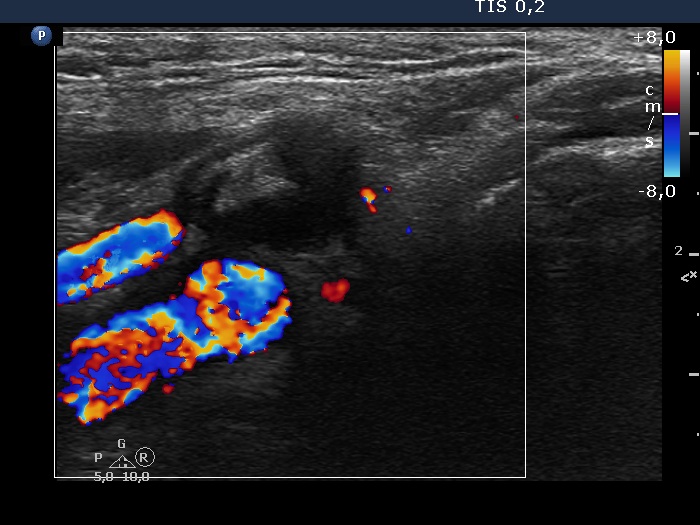
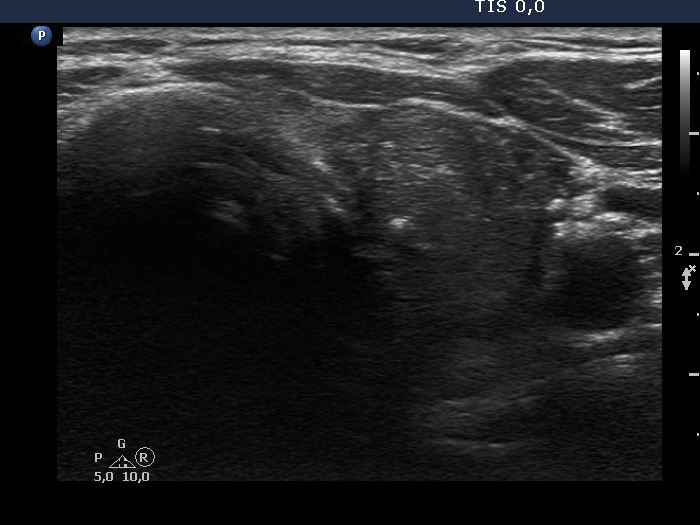
There was a conglomerate of lymph nodes 6 cm above the right lobe. The largest of these nodes was very hypoechoic but not cystic. There was another lymph node just above the right lobe. This node was composed of a very hypoechoic and an echonormal
part.
Cytology was performed from the nodules and from the conglomerate of lymph nodes in the right side of the neck and from the separate node just above the right lobe. The cytology resulted in thyroiditis not otherwise specified from the lesion in the right lobe, did in papillary cancer from the nodule in the left lobe. Necrotic material and benign, reactive-type lymphoid population was gained from the large, deeply hypoechoic neck mass and from the lymph node just above the right lobe, respectively. Wash-out thyroglobulin resulted in 0.1 ng/L from both lymph nodes.
Total thyroidectomy was performed. Histopathology disclosed papillary carcinoma in the left lobe. Except for the tumor in the left lobe, no other nodules were detected. Hashimoto's thyroiditis was described in the non-nodular parts of the thyroid. The lymph nodes in the right side of the neck proved to be benign with a pattern corresponding to a bacterial infection.
Comments.
-
This was a very unusual and challenging presentation, and despite histopathological results, the diagnoses at the time of the preoperative examination cannot be fully clarified.
It is evident that the patient had a lymph node infection, very likely of bacterial origin. The real question is the pathology of the large lesion in the right lobe. Beside Hashimoto's thyroiditis, acute and subacute thyroiditis should be also involved among the possibilities. -
The presentation of the lesion in the right lobe was very deceptive, it fully corresponded to papillary cancer.
-
The solitary lymph node just above the right lobe is also remarkable. The sharp contours stand against a bacterial infection while the heterogeneous pattern does for a metastatic origin.