
|
|
100 consecutive cases of papillary cancer - case 095
|
|





Clinical presentation: A 66-year-old man was referred for aspiration cytology of a thyroid nodule which was discovered on evaluation of mild hyperthyroidism. At the first exam 8 weeks ago, the laboratory test resulted in TSH 0.17 mIU/L, FT4 20.8 pM/L, FT3 8.01 pM/l.
Palpation: no abnormality.
Laboratory test: TSH 1.77 mIU/L, aTPO 0.5 U/mL, TSAb undetectable.
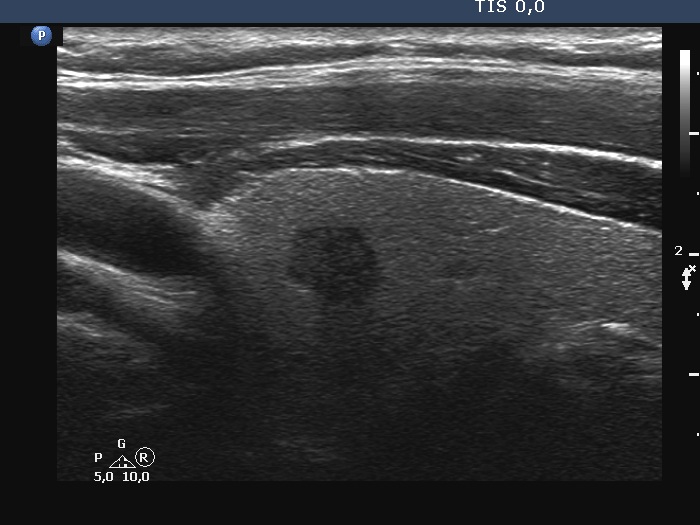
Ultrasonography. The thyroid was echonormal. There was a hypoechoic lesion in the right lobe. The lesion presented irregular borders and no vascularity. The size of the nodule was 7x6x8 mm, width, depth, length, respectively.
Cytology resulted in papillary cancer.
The patient's endocrinologist suggested surgery.
Left lobectomy was performed. Histopathology disclosed a T1a papillary cancer.
Comment.
-
Considering the size of the tumor and the age of the patient, a conservative approach could also have been undertaken.
-
It is worth comparing the test performed at a higher and lower frequency. It's not just obesity, it can worsen image quality (the patient had an average build). In men, probably the different consistency of connective tissue and/or muscle tissue often impairs the penetration of ultrasound.
-
The absolute measure of surface irregularities was not high, however, it is worth comparing the degree of undulations to the size of the nodule. I regard this as pathological lobulation.
-
In certain sections, the depth of the nodule exceeded the length but we must compare the largest depth to the largest length (and width) when judging the shape of a lesion.