
|
|
The borders of the nodule - case 1454doi: 10.24390/thyrocase1454bord.00
|
|


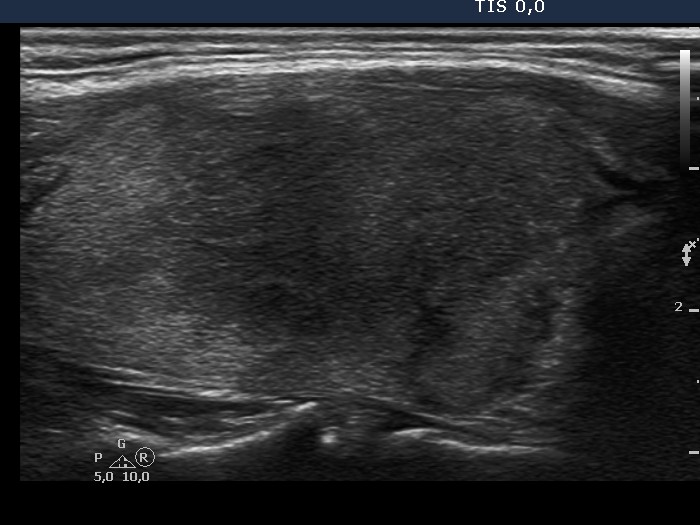















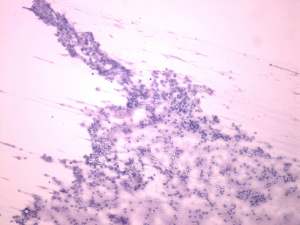
First examination (1st and 5th rows of images):
Clinical presentation: A 45-year-old woman presented with recurring neck pain and fever which have been lasting for 2 months. First her right thyroid was influenced. Antibiotics had no effect. The pain and fever have stopped after 3 weeks. 2 days before the present investigation the left thyroid became painful. She noticed fever again.
Palpation: Both thyroids were hard. The right lobe was tender, while the left one was painful.
Functional state: euthyroidism with TSH-level 0.34 mIU/L, FT4 17.9 pM/L, ESR 49 mm/H, CRP 38.1 mg/L.
Ultrasonography. There was a large hypoechogenic area in the right, while a relatively smaller one in the left lobe. Both presented blurred borders and decreased vascularization.
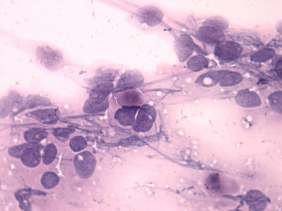
Cytological picture. Although there was no pathognomomic multinucleated giant cell on the smear, the cytological pattern corresponded to granulomatous, de Quervain's thyroiditis. The presence of thick colloid on the smear itself argues strongly against Hashimoto's thyroiditis.
Suggestion: steroid therapy for 6 weeks with gradually decreasing dose of methylprednisolone.
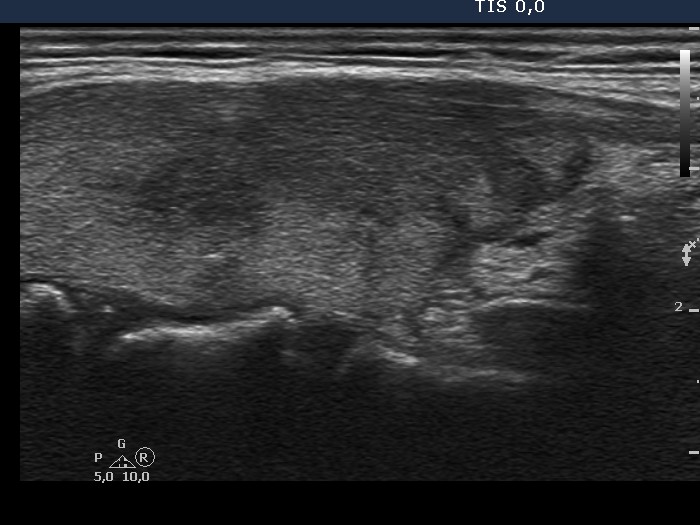
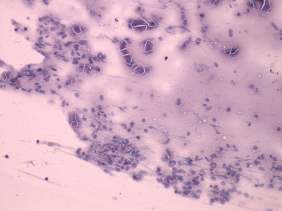
6 weeks after initial examination (2nd row of images):
Clinical presentation: The patient had no complaints except for fatigue and edema. Her complaints had stopped the day after administration of steroid.
Palpation: Both thyroids were firm and painless.
Functional state: euthyroidism with TSH-level 3.34 mIU/L, FT4 11.9 pM/L, ESR 18 mm/H, CRP 2,5 mg/L.
Ultrasonography. The right lobe and the proportion of the hypoechogenic areas in this lobe had decreased. The echo pattern in the left thyroid and the vascularization of both lobes were unchanged.
Suggestion: follow-up.
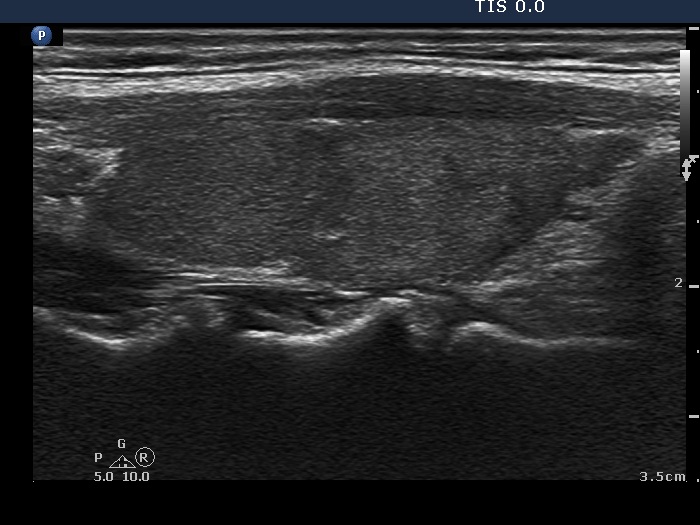
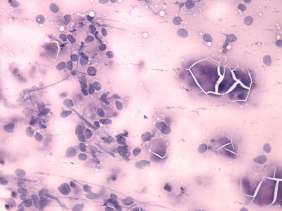
12 weeks after initial examination (3rd row of images):
Clinical presentation: The patient has noticed tenderness in the left side on the neck radiating to the ear and subfebrility for 2 weeks.
Palpation: The right thyroid was firm while the left was hard and painful.
Functional state: euthyroidism with TSH-level 0.67 mIU/L, FT4 13.0 pM/L, ESR 30 mm/H, CRP 11.8 mg/L.
Ultrasonography. The hypoechogenic areas in the right lobe have decreased further, while the hypoechogenic area in the left lobe increased significantly. The vascularization was normal in both lobes.
Suggestion: steroid therapy again for 4 weeks with gradually decreasing dose of methylprednisolone.
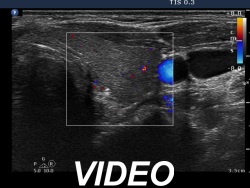
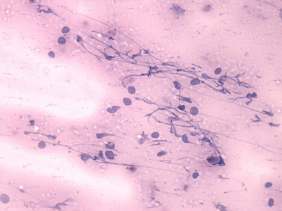
14 months after initial examination (4th row of images)
Clinical presentation: The patient had no complaints.
Palpation: The thyroid was not palpable.
Functional state: euthyroidism with TSH-level 3.41 mIU/L, FT4 11.2 pM/L, aTPO 0 U/mL, CRP 1.1 mg/L.
Ultrasonography. The thyroid was echonormal-minimally hypoechogenic. There were small, more hypoechogenic areas in both lobes, but the proportion of these fields were lower compared with the previous examination. The vascularization was average and decreased, right and left lobe, respectively.
Comments. The hypoechoic areas were blurred at the first, second and third examination, and also presented lobulated margins. These features are the usual presentation in subacute, de Quervain's thyroiditis.