
|
|
Intranodular hyperechogenic figures - case 1091
|
|












First examination (first row of images)
Clinical data: A 53-year-old woman was referred for evaluation of a nodule discovered on ultrasound screening. She had no complaints.
Palpation: There was a moderately firm nodule in the left thyroid.
Functional state: euthyroidism with TSH 1.06 mIU/L.
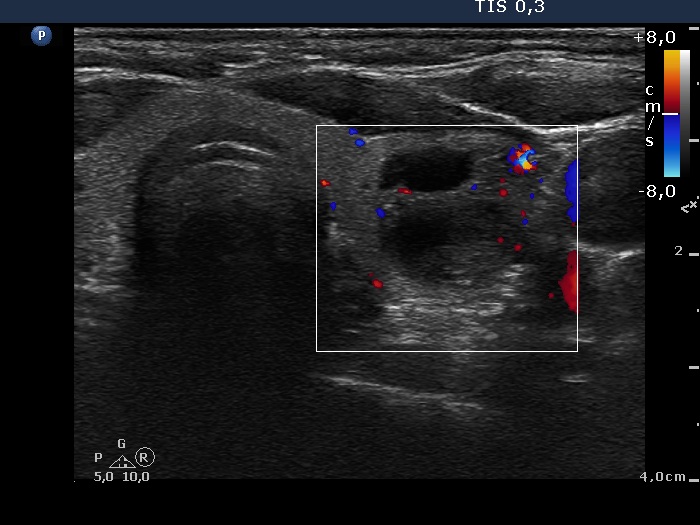
Ultrasound. The thyroid was echonormal. There was a mixed nodule in the ventral part of the left lobe. The lesion presented a moderately hypoechogenic solid part and different types of hyperechogenic figures including several caused by posterior back wall enhancement, comet-tail artifacts and non-specific figures corresponding to connective tissue.
One mL brown cystic fluid was aspirated. Cytological report: not diagnostic, cystic lesion.
A repeat cytology was advised 6 to 12 months later.
Second examination (second and third rows of images)
Clinical data: The patient had no complaints. Ultrasound was performed in another hospital a month ago and the radiologist told the patient that her nodule is highly suspicious because of the presence of microcalcifications. The lesion was categorized as a TIRADS 5 lesion.. The lesion was categorized as a TIRADS 5 lesion.
Palpation: unchanged.
Functional state: euthyroidism with TSH 0.85 mIU/L.
Ultrasound remained unchanged. Compared with the previous examination, the nodule has not increased in size.
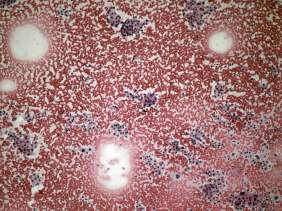
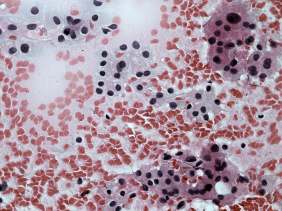
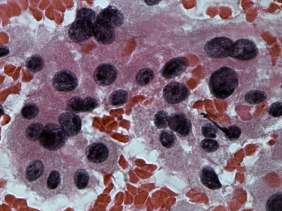
Aspiration cytology resulted in follicular proliferation.
Combined ultrasound-cytological diagnosis was benign follicular proliferation.
Follow-up was advised, however the patient decided to go on surgery because of the ultrasound report of the colleague.
A total thyroidectomy was performed and histopathology disclosed benign hyperplastic nodules.
Comments.
-
The cytological pattern itself is on the verge of a clearly benign proliferation and a follicular tumor: there was no colloid in the background and the ratio of isolated follicles was greater than in usual cases of a hyperplastic nodule. On the other hand the presence of pyknotic nuclei and degenerative forms as well the heterogeneous pattern suggested a non-tumorous origin.
-
The ultrasound presentation was also remarkable. Firstly, there are no signs of a capsule which decreases the likelihood of a follicular tumor to less than 5%. Secondly, the nodular area is composed of multiple discrete lesions which itself is a relatively specific sign of a hyperplastic nodule (see video).
-
The interpretation of tiny hyperechogenic granules is not always unequivocal and on our opinion the non-specific hyperechogenic granules are frequently misinterpreted as microcalcifications.
-
The TIRADS categorization shares several very serious problems, first of all because of the misuse by colleagues. To describe a nodule on the ultrasound report as moderately suspicious or highly suspicious causes more damage than all the system's benefit. Be aware that a patient is a human being with his or her distress caused by the medical examination itself. Why further increase the anxiety? His or her nodule will be soon aspirated if necessary. No one reporting system can replace the correct interpretation based on the practice.
-
This case illustrates the issue of differential diagnostic or intranodular figures: granules occurring in the presence of connective tissue, colloid crystals and figures caused by posterior back wall enhancement all may be misinterpreted as microcalcifications as happened in this patient.
-
The above listed points may be disputed but we think that considering all of the conditions described above, the choice of a total thyroidectomy was a failure.