
|
|
Intranodular hyperechogenic figures - case 386
|
|



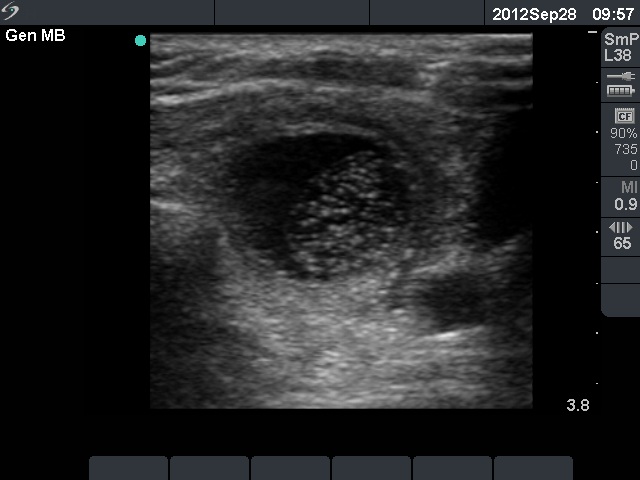



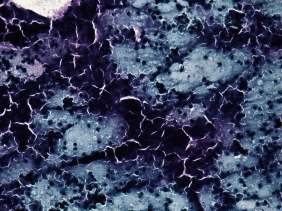



First examination (1st row of images)
Clinical presentation: A 60-year-old woman was referred for a follow-up investigation. She has been known to have a nodule in the left lobe for 7 years. She had 'lump in the throat' feeling.
Palpation: a nodule in the left lobe.
Functional state: euthyroidism (TSH-level 2.95 mIU/L).
Ultrasonography: The right thyroid was intact. There was a hypoechogenic nodule in the left lobe. Compared with the formed examination, the nodule increased in volume by 38%.
Cytological diagnosis: benign colloid goiter.
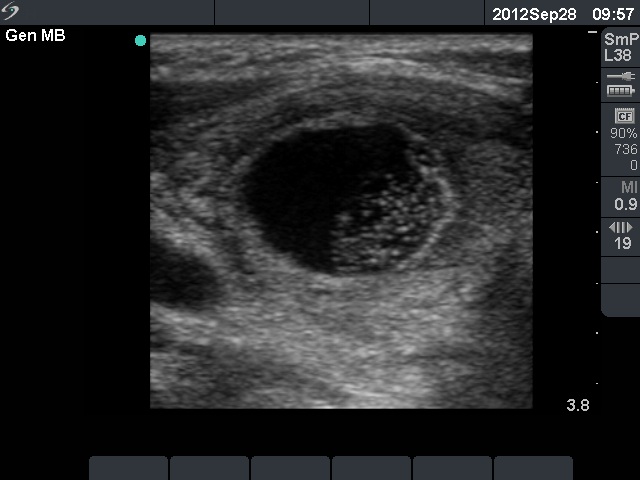
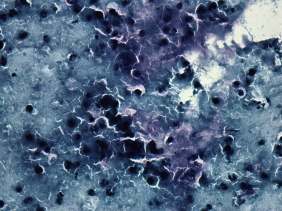
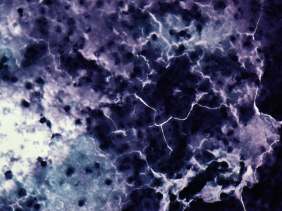
Second examination 3 weeks later (2nd and 3rd rows of images)
Clinical presentation: The patient told that her right thyroid became painful and she had fever. Her complaints began for 3 days. Antibiotics were administered, but her complaints remained unchanged.
Palpation: The whole left thyroid was hard and painful.
Laboratory tests: granulocytosis (11 G/L) and elevated CRP level (23.8 mg/L).
Ultrasonography: The thyroid was unchanged except for increase in size of the nodule in the left lobe. The lesion became cystic and contained multiple hyperechogenic granules corresponding to protein-rich structures. The nodule was avascular.
We aspirated 5 ml purulent cystic fluid. Cytological diagnosis: acute inflammation.We changed the antibiotics.
Third examination 1 week later (4th row of images)
Clinical presentation: The patient had no complaints.
Palpation: The thyroid was painless but already very firm.
Laboratory investigation: granulocytosis and CRP level decreased, 9.6 G/L and 10.7 mg/L, respectively.
Ultrasonography: the nodule became smaller and the cystic part has not refilled.
Fourth examination 30 month after the initial examination (5th row of images)
Clinical presentation: The patient had no complaints after the last visit. We met her three times. Laboratory tests remained normal.
Palpation: no abnormality.
Functional state: euthyroidism (TSH-level 2.71 mIU/L).
Ultrasonography: The thyroid was echonormal. According to the previously inflamed nodule, there was a much smaller hyperechogenic lesion in the left lobe.
Comments.
-
We performed around 50,000 FNAs, it means around 150,000 punctures of thyroid. Three cases occurred when 1 to 3 weeks after the examination the patient presented acute inflammation.
-
Note the hyperechogenic, protein-rich structures at the time of acute inflammation.
-
Naturally, this case is not a true purulent thyroiditis, because only the nodule presented the signs of inflammation while the extranodular thyroid remained intact.
-
Although the patient suffered a painful disease, this attack had the advantage that her nodule decreased significantly in size thanks to the inflammation.