
|
|
The echogenicity of the nodule - case 2169
|
|




Clinical presentation: A 38-yr-old woman requested evaluation. She was treated for subacute de Quervain's thyroiditis with methylprednisolone 17 years ago. Five years later, despite normal TSH level, thyroid replacement therapy was initiated on complaints suggesting hypothyroidism. In the last 3 weeks she occasionally felt pain in the left side of the neck. Her body temperature remained normal.
Palpation: The left lobe was hard and tender on palpation.
Laboratory tests: TSH 1.26 mIU/L on daily 75 microgram levothyroxine, CRP 1.5 mg/L (normal value < 5), aTPO 0.5 U/mL.
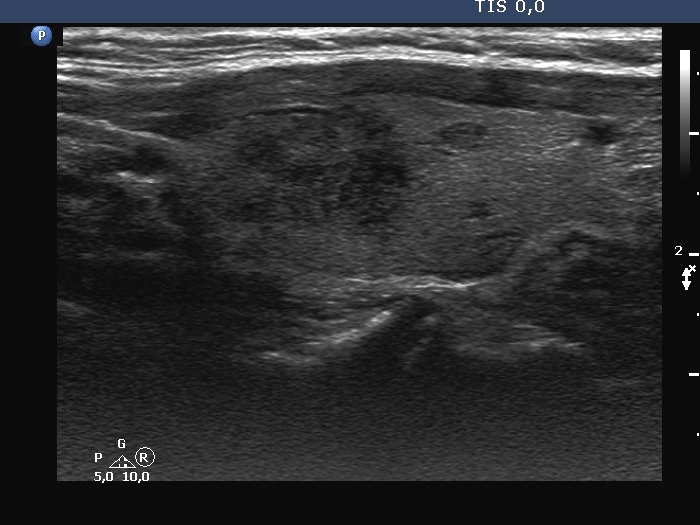
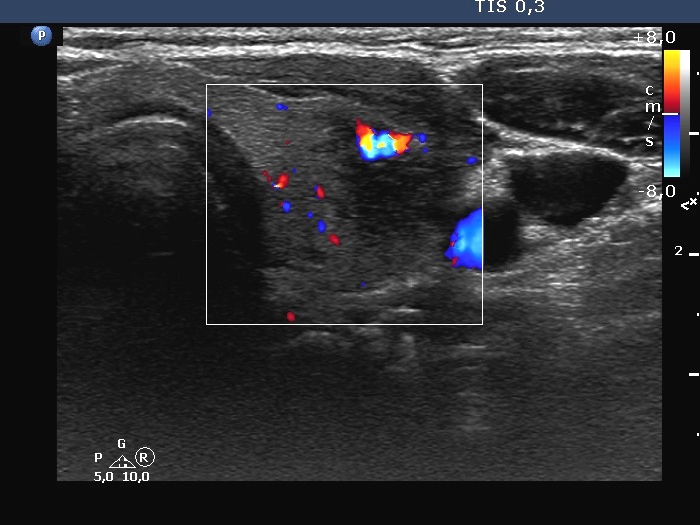
Ultrasonography. The thyroid was minimally hypoechoic. There was a small, discrete lesion in the upper pole of the right lobe. The left lobe had a larger and several tiny hypoechogenic lesions. The large lesion presented partly blurred, partly lobulated margins.
Cytology was performed from the large hypoechoic lesion in the left lobe and resulted in subacute, de Quervain's thyroiditis.
Comments.
- This is a highly unusual case. De Quervain's thyroiditis recurs only exceptionally years after an attack. In our practice based on the management of more than 700 cases, the late recurrence rate is in less than 1%. The second unusual circumstance was that the patient was treated unnecessarily with levothyroxine. And last, but not least, the laboratory data did not support the diagnosis of de Quervain's thyroiditis, at all. Neither the normal CRP levels nor the lack of thyroid dysfunction. On the normal CRP level, the diagnosis of de Quervain's thyroiditis could be questioned.
- The hypoechoic lesion in the left lobe has lobulated, spiculated margins.
- In judging echogenicity, it may be worth mentioning that in the case of de Quervain's and Hashimoto's thyroiditis, discrete lesions are often heterogeneous. However, the reason for this is that the intact, less hypoechoic parenchyma is infiltrated by inflammation.