
|
|
TIRADS - case 1281
|
|



Clinical presentation: A 32-yr-old woman was referred for evaluation of a mass in the thyroid which was noticed by the patient herself.
Palpation: a firm nodule in the right lobe.
Laboratory tests: TSH 0.34 mIU/L, aTPO 44 U/mL, TSAb below 0.8 U/L.
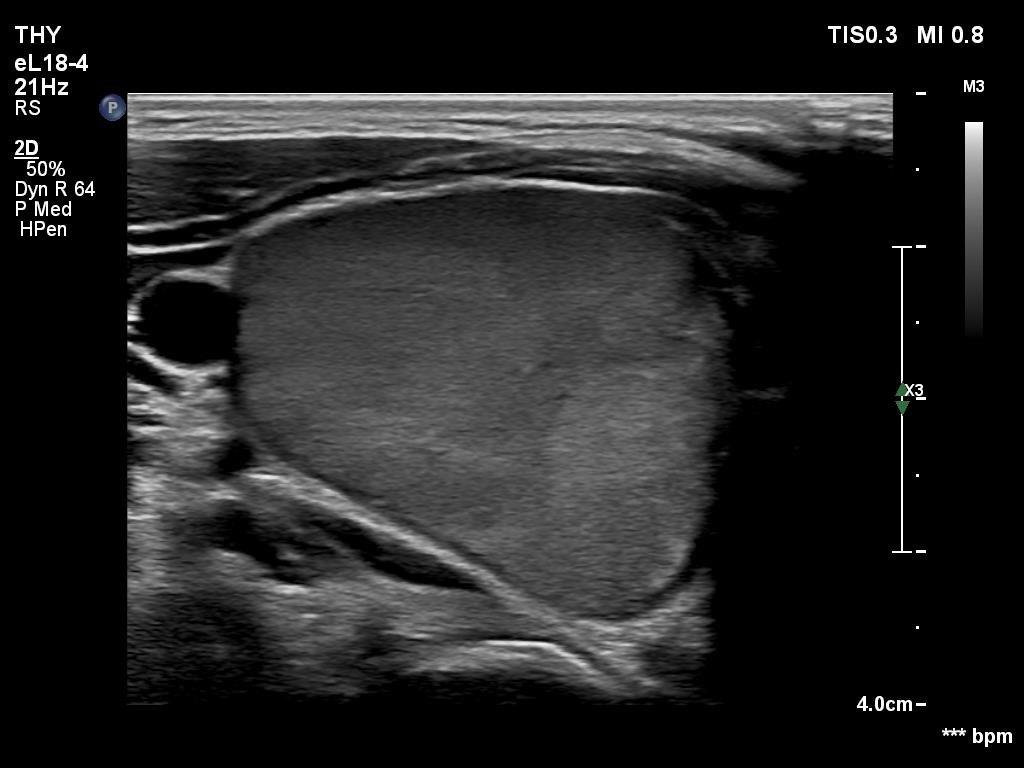
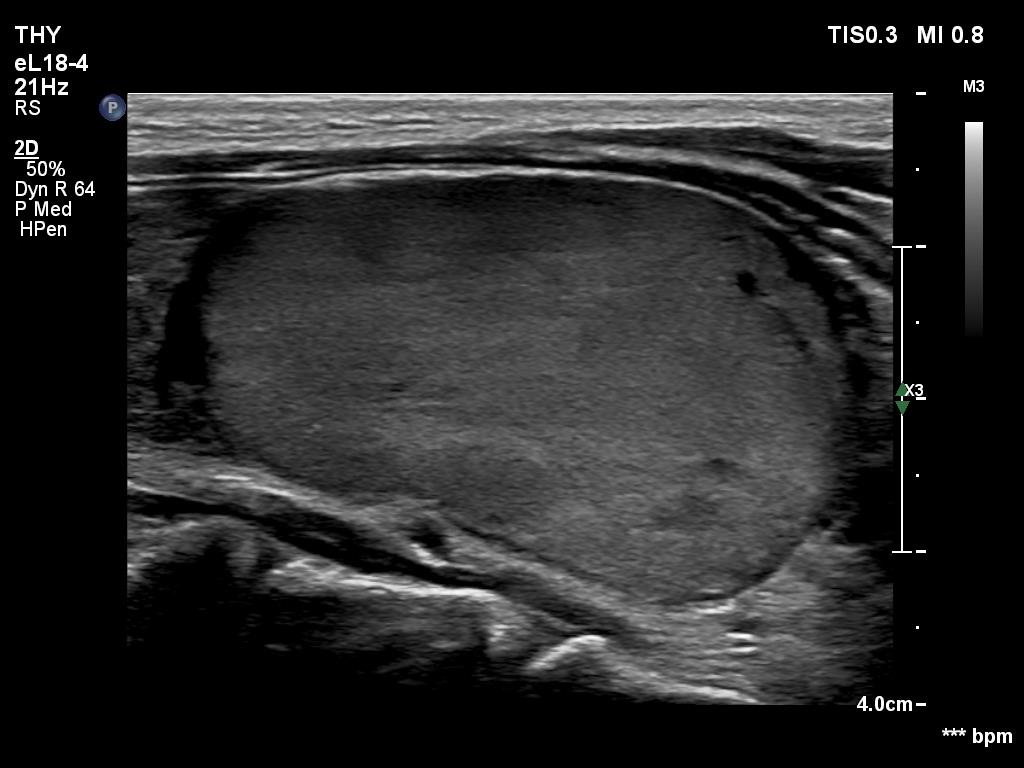
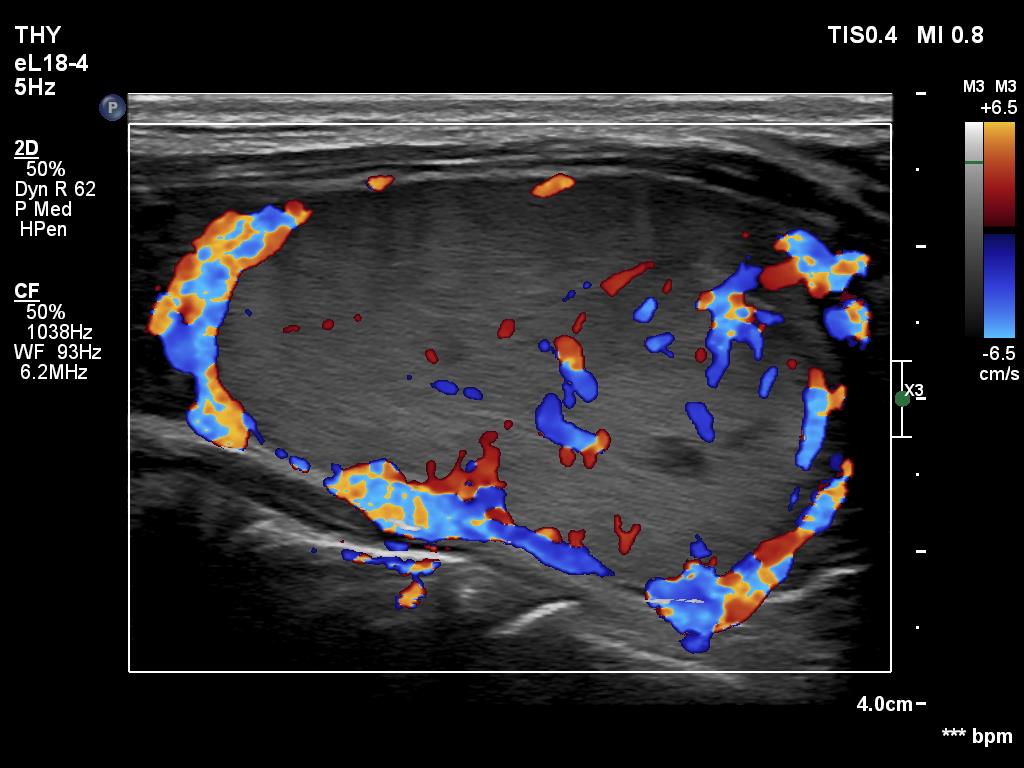
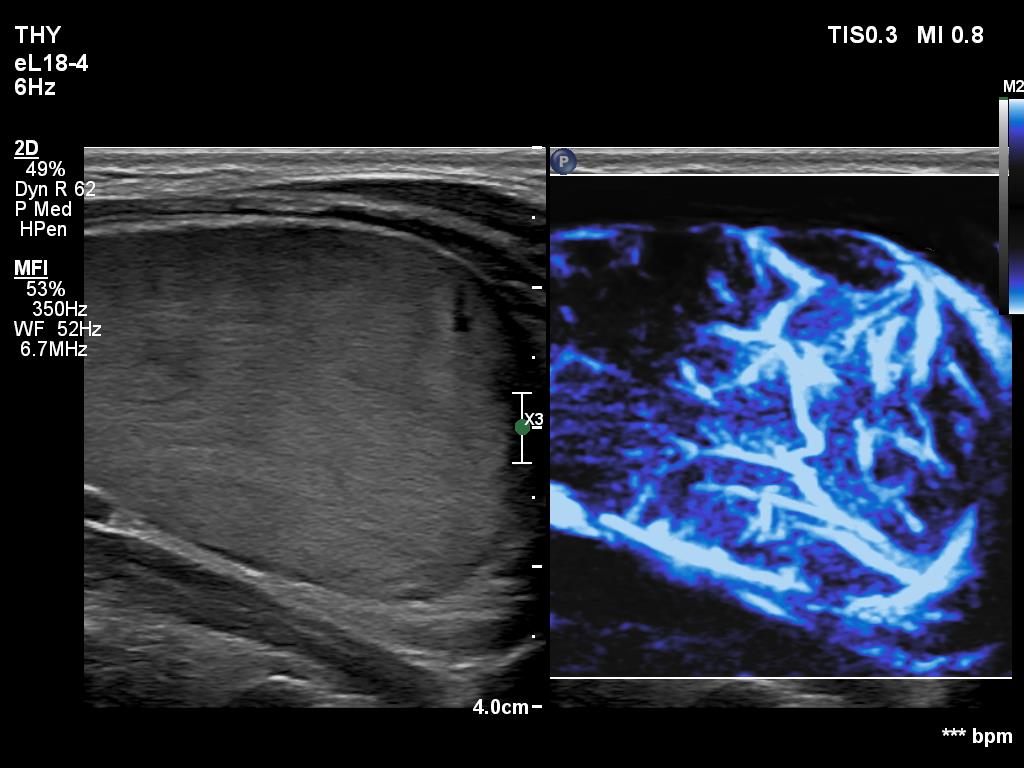
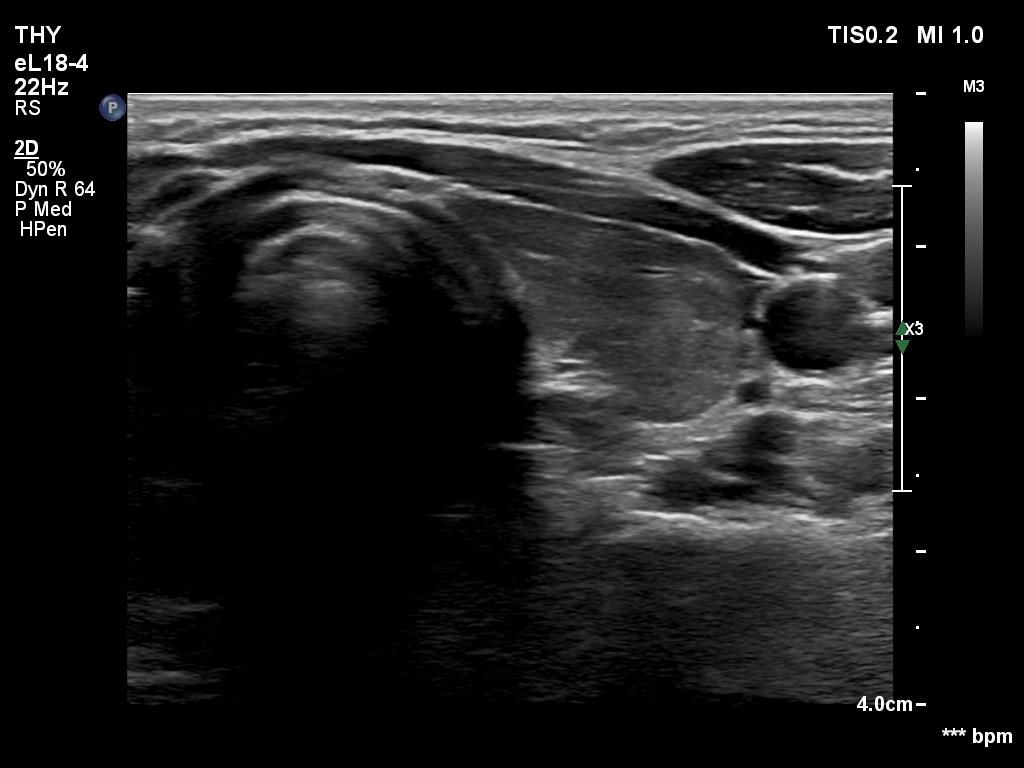
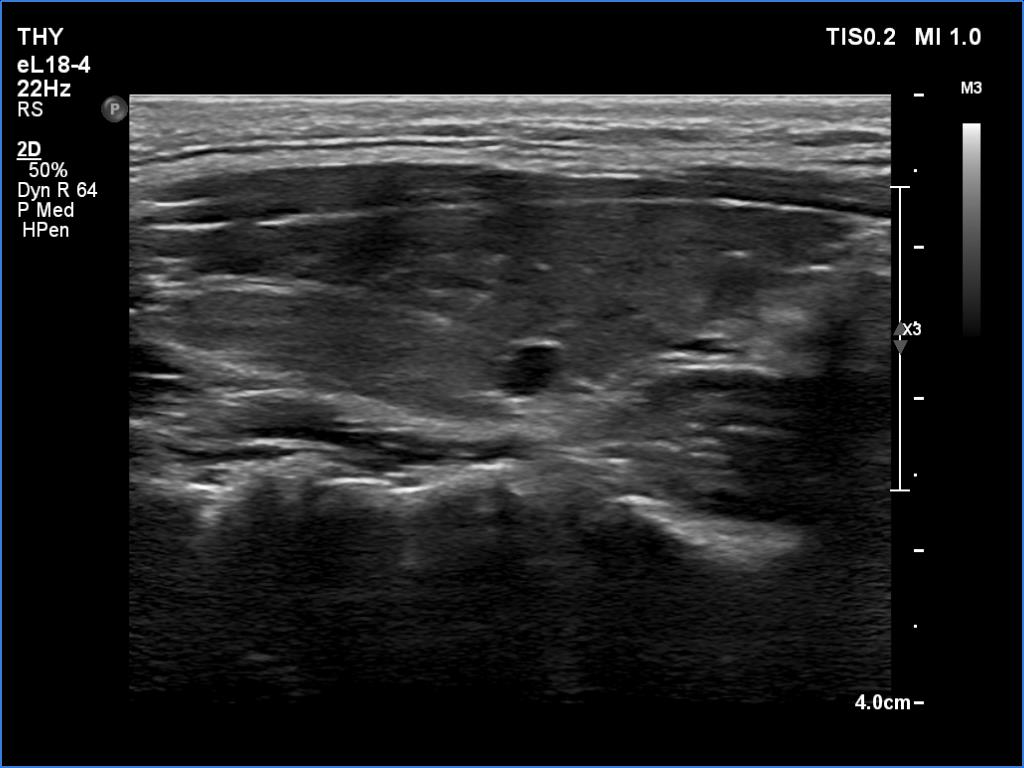
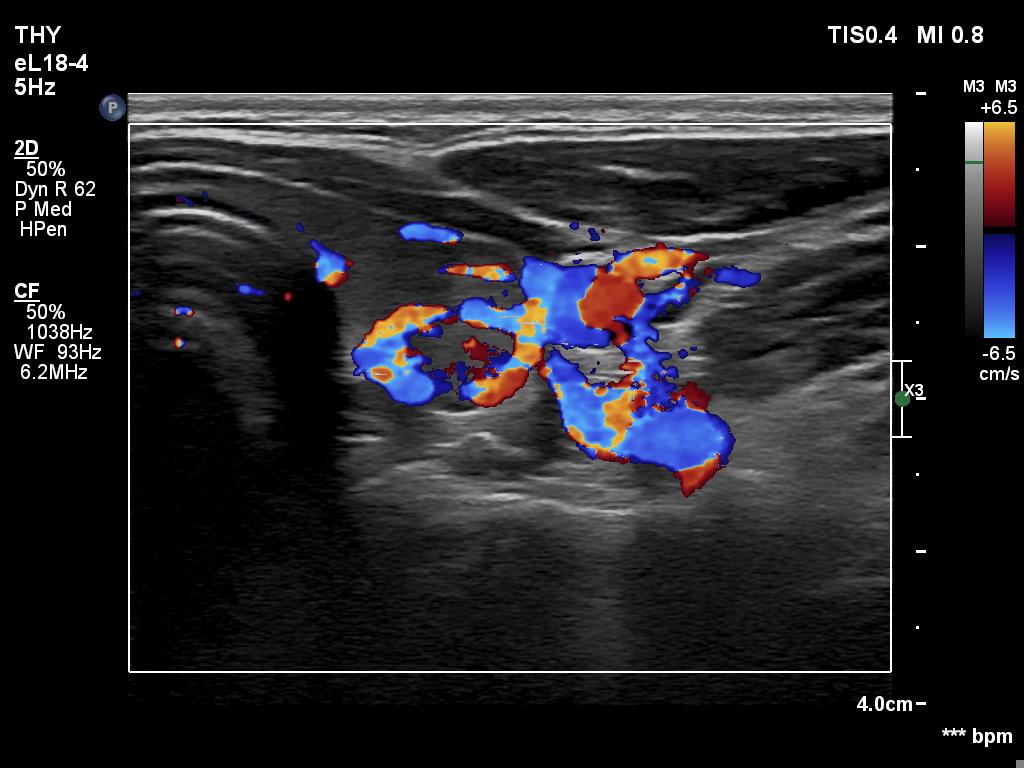
Ultrasonography. The thyroid was moderately hypoechoic. A large nodule occupied almost the entire right lobe. The nodule was more echogenic compared to the extranodular tissue. If we compared the nodule' echogenicity to that of a normal, healthy thyroid, then the nodule should be regarded as a dominantly minimally hypoechoic, heterogeneous lesion. The nodule presented both perinodular and intranodular vascularity.
The cytology corresponded to Hashimoto's thyroiditis.
Our combined sono-cytological diagnosis was follicular tumor.
A right lobectomy was advised.
Histopathology disclosed an oxyphilic adenoma corresponding to the nodule while Hashimoto's thyroiditis in the extranodular part.
Comments.
-
Such ultrasound presentation is very characteristic of a follicular tumor: a solitary large nodule showing both halo and perinodular vascularity is the typical ultrasound presentation of a follicular tumor.
-
The cytology did not show any sign of a follicular tumor, it fully corresponded to Hashimoto's thyroiditis.
-
Regarding the classification of the nodule, I refer to comments above. The nodule is a TIRADS 3 lesion if the reference tissue is the extranodular part while it is a TIRADS 4 lesion if the reference tissue is the healthy thyroid.