
|
|
Parathyroid lesions - case 447
|
|














Clinical data: A 40-year-old woman was referred for evaluation of a nodule detected on screening. She had no complaints.
Palpation: no abnormality.
Laboratory test: TSH 1.77 mIU/L.
Ultrasonography. The thyroid was echonormal. There was a hypoechogenic nodule presenting microcalcifications and irregularly increased intranodular blood flow in the central part of the right lobe while a more hypoechogenic lesion in the lower lateral part of the right lobe. The latter displayed irregular borders and an increased intranodular vascularity. The latter mass was not described on previous ultrasound examination and was hard to differentiate from muscle fiber.
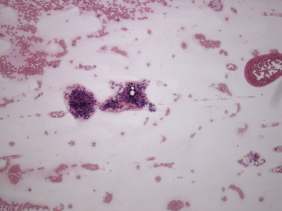
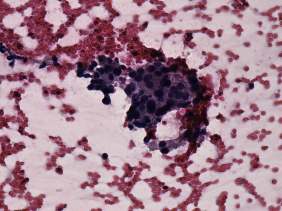
Aspiration cytology of the nodule in the central part of the right thyroid resulted in benign colloid goiter while that of the lesion in the lower pole of the right thyroid resulted in benign lesion which might correspond to parathyroid adenoma.
Wash-out was thyroglobulin was low (1.06 mg/L), while wash-out parathormone resulted in 80.1 pg/mL. (It was performed from the suspected parathyroid lesion.)
Further laboratory tests: calcium 2.85 mM/L, phosphorus 0.84 mM/l, parathormone 118.2 pg/mL (normal value: 15-66).
Scintigraphy disclosed parathyroid lesion corresponding to the mass in the lower-ventral part of the thyroid.
Left lobectomy was performed with the removal of the right lower parathyroid. Histopathology: benign, hyperplastic nodule and parathyroid adenoma corresponding to the right lower parathyroid.
Comments.
-
This case study illustrates a rare exception when the ultrasound screening was clearly to advance of the patient and led to discovery of hyperparathyroidism.
-
The thyroid lesion presented a suspicious ultrasound pattern.
-
If we analyze the images of the lower pole of the thyroid, the discrimination of the thyroid, the sternocleidomastoid muscle and the parathyroid lesion seems to be not difficult. However, to find the adequate section to discriminate the parathyroid lesion from the sternocleidomastoid muscle was not a simple task and required a thorough examination.