
|
|
Consecutively operated patients with autoimmune thyroid disease - case 38 (54)
|
|








Clinical presentation: A 45-year-old man was referred for evaluation of a recurrent hyperthyroidism. He has been treated for hyperthyroidism for two years.
Palpation: The left lobe was enlarged and had a firm nodule.
Laboratory tests: TSH 0.001 mIU/L, FT4 43.2 pM/L, TSAb 3.9 U/L (normal value < 1.5).
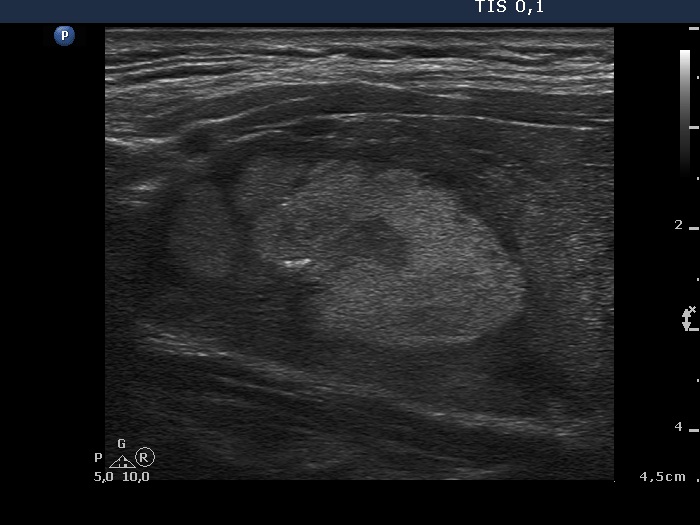
Ultrasonography. The thyroid was moderately hypoechogenic and contained at least three nodules. The vascularization was increased in the extranodular part.
Cytology of the largest nodule in the left lobe resulted in benign colloid goiter.
Surgery was advised. Histopathology disclosed benign hyperplastic nodules in both lobes and chronic lymphocytic thyroiditis.
Comment.
-
Usually if we see a lesion with infiltrative borders, it is evident that the lesion itself is responsible for the invasion. However, in the event of an underlying thyroiditis, the situation might be completely the opposite, as happened in this case. The nodule borders seem to be irregular, but this is caused by the infiltration of the underlying thyroiditis. In essence this is not a pathological lobulation or spiculation of the nodule-like lesion.
-
Although the discrete lesions have hypoechoic islets, they are the result of the underlying thyroiditis. It means that these lesions are not heterogeneous.