
|
|
100 consecutive cases of papillary cancer - case 011
|
|

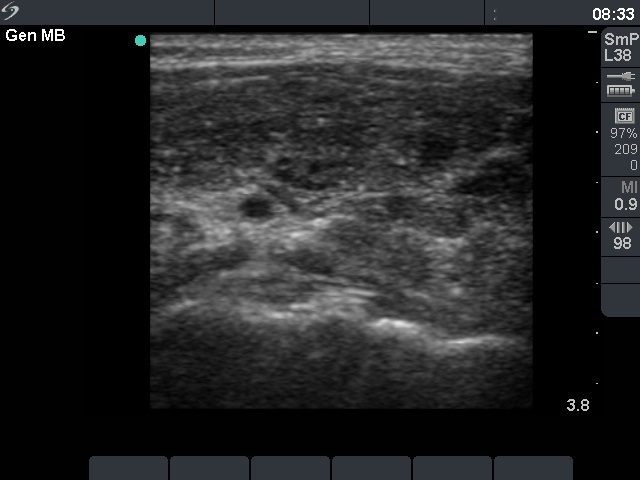
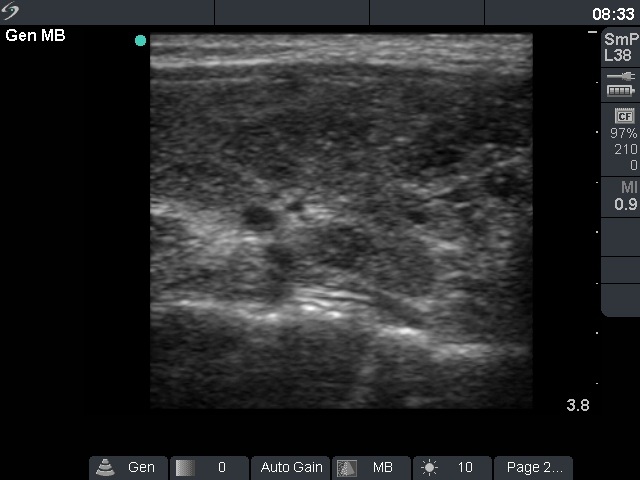

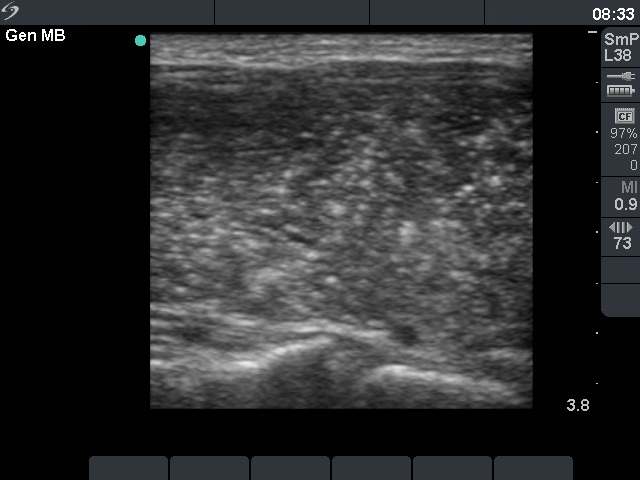
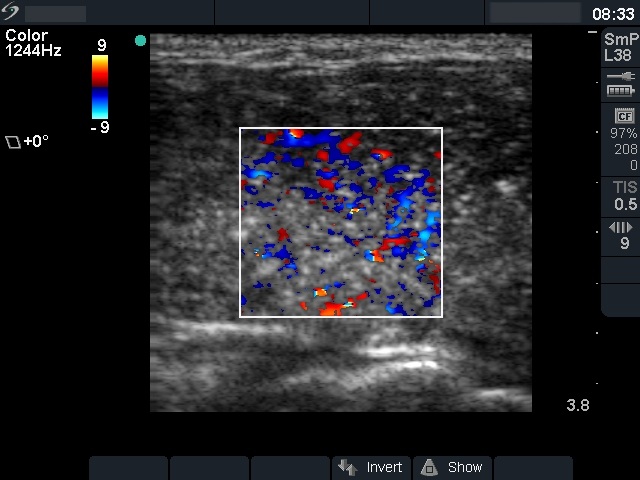

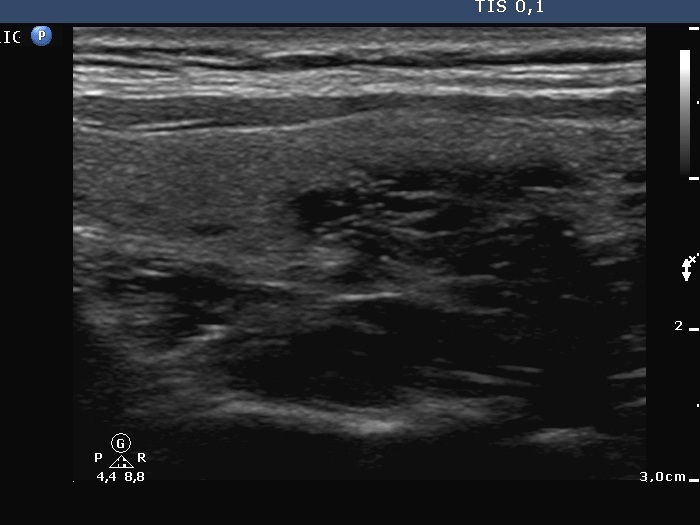





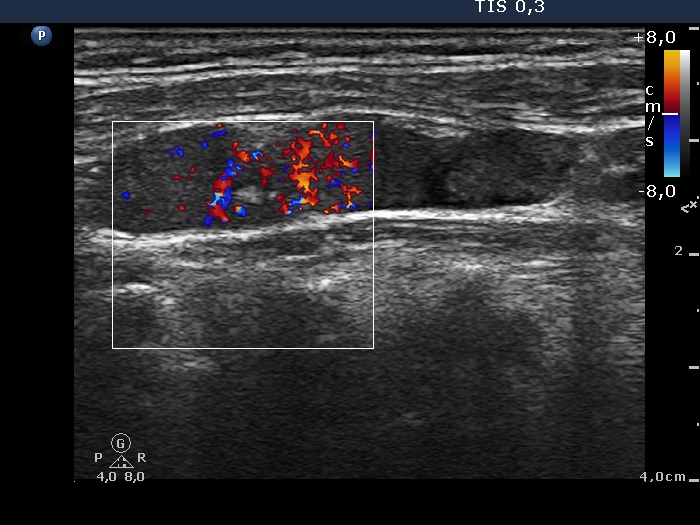
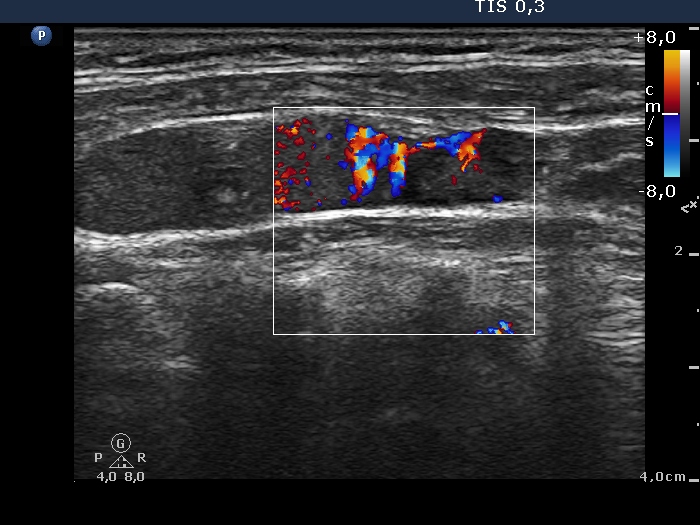


First examination (first row of sonographic images):
Clinical presentation: A 33-year-old woman was referred for evaluation of typical complaints suggesting hyperthyroidism.
Palpation: Both lobes were enlarged.
Functional state: hyperthyroidism (TSH undetectable, FT4 42.2 pM/L, FT3 above 46 pM/L).
Ultrasonography. The thyroid was diffusely hypoechogenic. The vascularization was increased. The left lobe was significantly more inhomogeneous than the right lobe. Compare the first two index pictures in the first row with the third and fourth one, right and left lobe, respectively.Thyrostatic drug was administered for 12 months, thereafter the drug was discontinued.
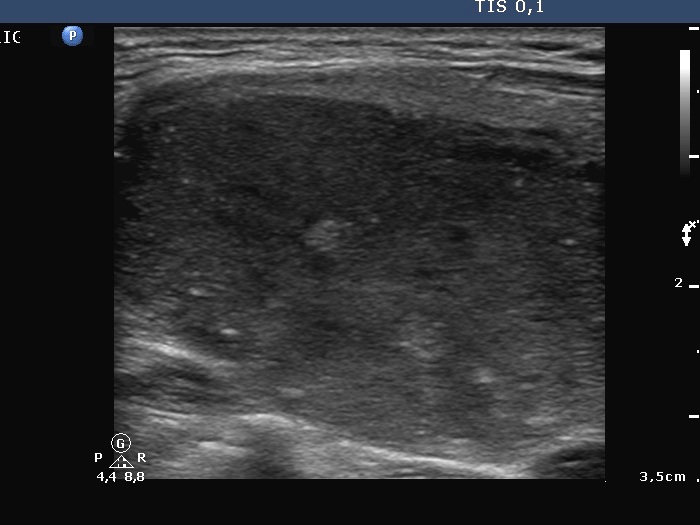
Follow-up examination 17 months after first visit (second and third rows):
Clinical presentation: The patient was well. She came to sonographic follow-up suggested at her first visit.
Palpation: a hard nodule in the upper part of the left lobe.
Functional state: subclinical hyperthyroidism (TSH undetectable, FT4 21.1 pM/L, FT3 6.68 pM/L).
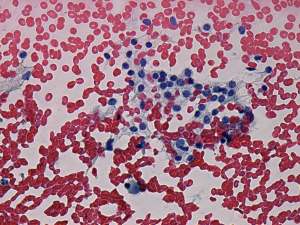
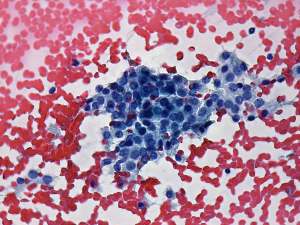
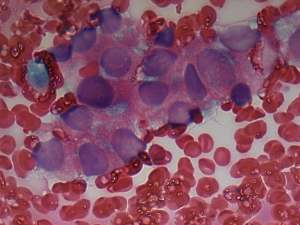
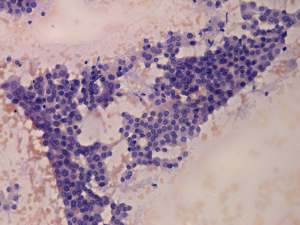
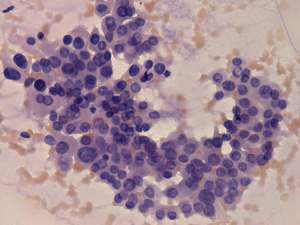
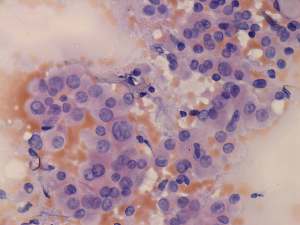
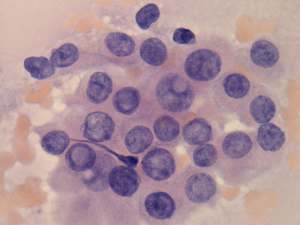
Ultrasonography: The echogenicity index of the thyroid was 50%. The vascularization was not significantly increased. There was a large hypoechogenic, inhomogeneous nodule in the upper part of the left lobe. Both the intranodular and the perinodular blood flows were increased.Cytological picture: There was no colloid in the background. Follicular cells were found in microfollicles and displayed anisonucleosis and cytoplasmic vascularization. A few cells contained grooves. There was an atypical cell group at one edge of the smear. It was composed of around 20 enlarged, atypical cells. This structure resembled a cluster of papillary cancer.
Cytological diagnosis: suspicion of a well-differentiated thyroid cancer.
Histopathology: papillary cancer according to the nodule in the left lobe with multiple small metastatic foci in the right thyroid. One of 11 lymph nodes of the neck contained metastasis.
Follow-up examination 4 weeks after surgery (fourth and fifth rows):
Radioiodine treatment was planned. The patient visited us to get information about the prognosis of her disease.
Palpation: no abnormality.
Ultrasonography: There was no parenchyma in the thyroid beds. There were multiple enlarged lymph nodes in the lateral side of the neck. One of them very close to the thyroid seemed to be benign, reactive, but there was a chain of atypical, suspicious lymph nodes next to the strernocleidomastoid muscle.
Cytology: papillary cancer.
The patient was reoperated. Histopathology disclosed metastatic foci in the lymph nodes. 6 weeks later she underwent radio-iodine treatment.
Comments.
-
It seems to be a reasonable assumption that papillary cancer had been already present at the first investigation. It was very unusual that the left thyroid was significantly more inhomogeneous than the right lobe. The former contained relatively large hyperechogenic granules, however, there were no discrete circumscribed lesion in the left lobe.
-
It is worth analyzing the video recorded at the second examination. Both the nodule and the extranodular part present fibrotic changes, moreover the inhomogeneity of the extranodular part is more pronounced than that of the nodule.
-
The performance of ultrasound may have role after surgery (thyroidectomy and appropriate lymphadenectomy) but before radioiodine treatment. Ultrasound examination can reveal insufficiency of surgery in around 10 to 20% of such cases. Most of these cases occur when either the surgeon performed the exploration is relatively inexperienced or in cases where the diagnosis has not been made preoperatively and therefore the appropriate lymphadenectomy was not performed.