 |
|
 |
Table 6 Technical issues
|
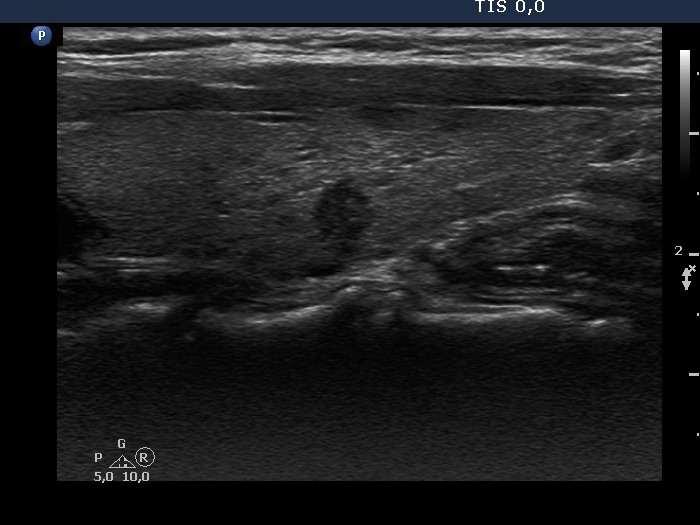
There are several reasons for an improper visualization of the echogenicity. The most important problem is that the transducer cannot be fit to the neck of the patient all along. Dorsal to those fields which are not properly fit, the echogenicity decreases. There are anatomical structures which influence the echogenicity of the thyroid, these are cystic areas and macrocalcifications. In the former, the echo signal gets amplified while in the latter, it decreases.
|
Transverse scan |
Longitudinal scan |
 |
 |
 |
 |
Great proportion of the nodule' borders are indistinctive. However, the cause of the blur is very likely not pathological. First, the focus was set wrongly (red arrow), therefore the dorsal part of the nodule is difficult to judge (yellow arrow in the transverse scan). Second, the upper and lower parts of the nodule are blurred (yellow arrows in the longitudinal scan) because of the placement of the transducer. It can be difficult to properly fit the probe all along to the patient's neck.
|
|
|
|
Transverse scan |
Longitudinal scan |
 |
 |
|
|
In contrast with the images of transverse scan where the borders of the nodule seem to be ill-defined, longitudinal scan images present sharp borders. The difference is caused by the placement of the transducer: in the event of transverse scanning to fit the probe all along parallel with the neck structures can be more difficult because of anatomical situation. Note that the images differ not only in nodule' borders but even in the echogenicity of the lesion and the extranodular part.
|
|
|
 |
 |
The thyroid parenchyma is echonormal in the ventral part while moderately hypoechoic dorsal to the iso/hyperechoic nodule. Thicker the nodule in the section, darker the non-nodular thyroid dorsal to the lesion.
|
|
|
Transverse scan |
Longitudinal scan |
 |
 |
 |
 |
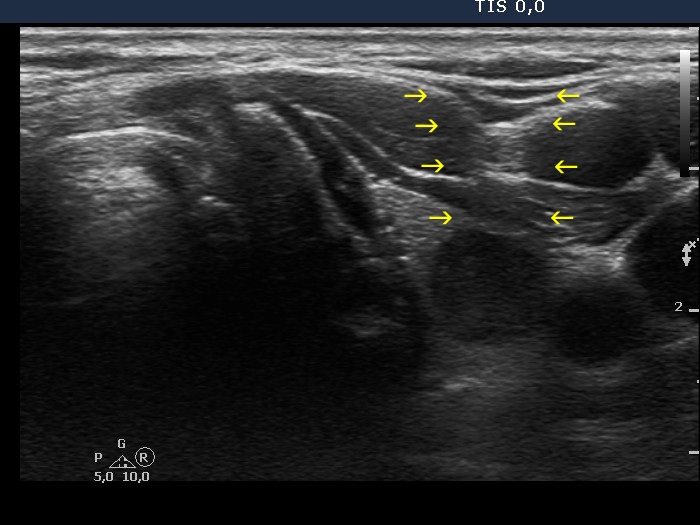
Two technical issues are demonstrated in this case. The dark band medial (transverse scan) and upper (longitudinal scan) to the nodule starts ventral to the thyroid. It is caused by the improper fitting of the transducer to the neck of the patient. The non-nodular part dorsal to the nodule is more echogenic. This is similar to the phenomenon that the signal behind a cyst gets amplified and it is not infrequently observed in the event of deeply hypoechoic nodules.
|
|
|
Parathyroid carcinoma (histology) - case 755 |
Transverse scan |
Longitudinal scan |
 |
 |
This is a hypoechoic lesion which proved to be a parathyroid carcinoma which was located in the lower pole of the left lobe. In the transverse view, the tumor is brighter than the strap muscle while the situation is the opposite in the longitudinal scan.
|
|
Parathyroid carcinoma (histology) - case 500 |
Transverse scan |
Longitudinal scan |
 |
 |
 |
 |
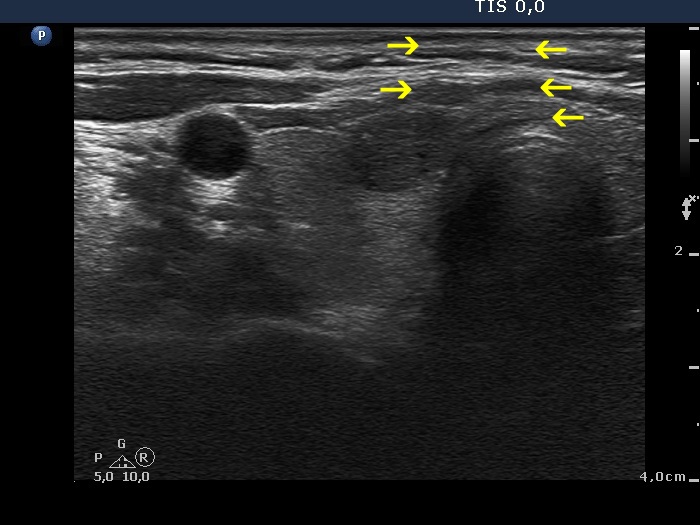
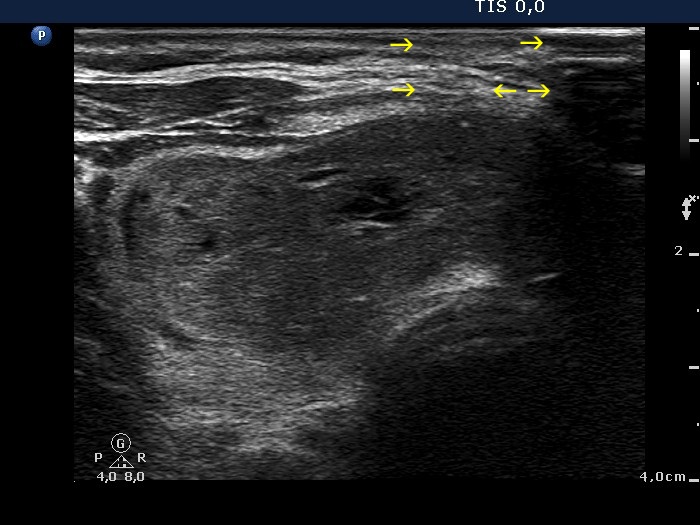
The nodule is clearly hypoechoic. The degree of hypoechogenicity cannot be judged on transverse scan because there is a hypoechoic band ventral to the nodule (yellow arrows). Note the amplification of the echo dorsal to nodule (red arrows).
|
|
Follicular adenoma (histology) - case 33 |
Transverse scan |
Longitudinal scan |
 |
 |
 |
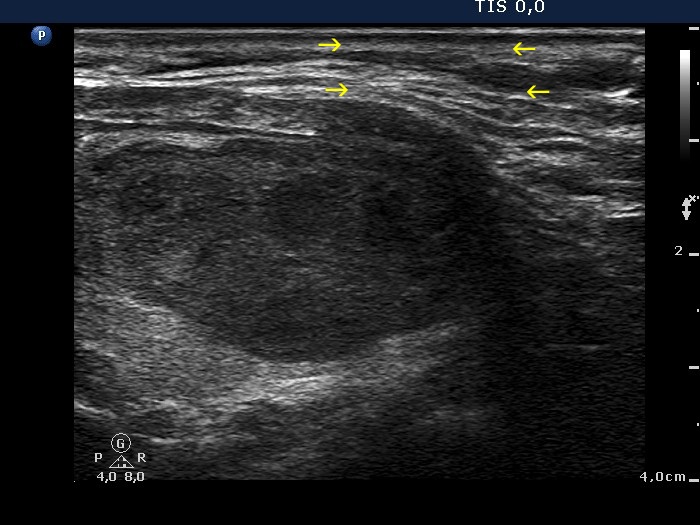 |
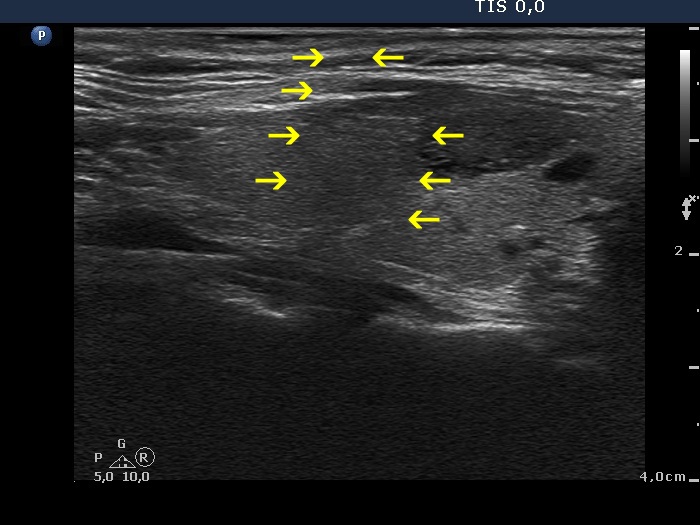
This nodule is moderately hypoechoic (see the video). The deeply hypoechoic parts of the lesion are the consequence of improper fitting of the ultrasound probe to the neck of the patient (yellow arrows).
|
|
|
|
 |
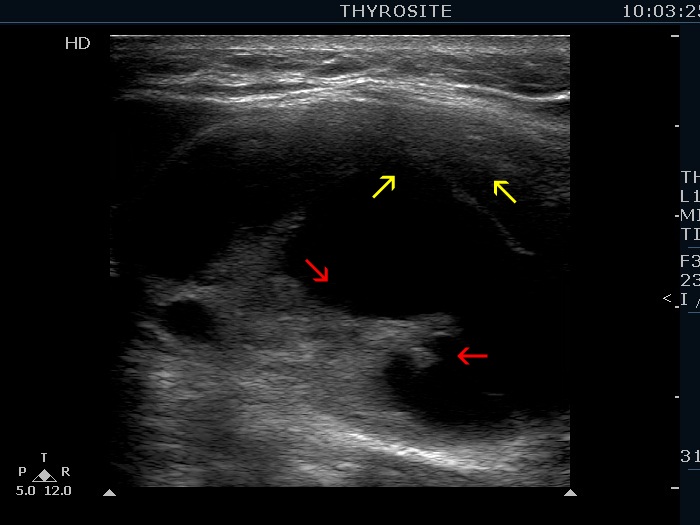 |
Let's compare the solid areas located in the ventral (yellow arrows) and in the dorsal part (red arrows) of the cystic nodule. The latter is more echogenic because the echo signal gets amplified dorsal to the cystic fluid.
|
|
|
|
Transverse scan |
Longitudinal scan |
 |
 |
The echogenicity of the nodule differs on transverse and longitudinal scan because of technical reasons. In this case, the probe was difficult to fit to the neck of the patient on transverse scan, therefore this view was the deceptive one.
|
|
|
|
Transverse scan |
Longitudinal scan |
 |
 |
 |
 |
Depending on how accurately we were able to fit the transducer to the patient's neck, the echogenicity of the nodule was different. If we face a technical problem which alters the nodule' echogenicity, the brightest (most echogenic) pattern corresponds to the reality. The nodule showed taller-than-wide sign.
|
| |
|
|
|