
|
|
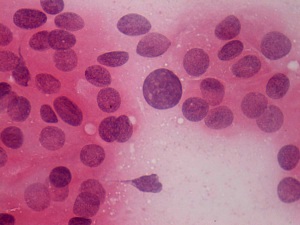
The borders of the nodule - case 469
|
|










Clinical presentation: A 28-year-old woman was referred for evaluation of vertigo and hair loss.
Palpation: Both lobes were moderately firm. No nodule could be palpated.
Functional state: subclinical hypothyroidism with TSH-level 7.07 mIU/L, FT4 14.0 pM/L, aTPO 496 U/mL.
Ultrasonography: The thyroid lobes were minimally-moderately hypoechogenic. There were two more hypoechogenic lesions next to each other in the dorsal part of the right lobe. In addition to, a hypoechogenic lesion with invasive borders was found in the central part of the left lobe. The latter nodule presented the so-called starry sky phenomenon and an increased intranodular vascularization.
Cytology was performed. The patient felt an unusual fear from aspiration. I told her that I plan to aspirate her three times, but she permitted me only one aspiration. As the video demonstrates we successfully targeted the lesion in the left lobe. The cytological pattern corresponded to Hashimoto's thyroiditis. Intraoperative imprint smears are demonstrated in this case study.
Final combined clinical-ultrasound-cytological diagnosis was subclinical hypothyroidism caused by Hashimoto's thyroiditis and suspicion of papillary carcinoma with greater than 50% risk of malignancy. Considering the ultrasound presentation, we told the patient that irrespectively of the result of the cytology surgery cannot be avoided.
Surgery was performed. Intraoperative frozen section disclosed papillary carcinoma in the left lobe. Histopathology disclosed multifocal papillary carcinoma corresponding to the lesion in the left lobe and Hashimoto's thyroiditis. No nodule was found in the right lobe.
Comments.
-
On such ultrasound presentation (starry sky phenomenon, increased intranodular blood flow, irregular borders in a hypoechogenic nodule) the risk of a papillary carcinoma is greater than 50%.
-
This case illustrates the difficulty to gain adequate material from a vascularized tumor.
-
In the everyday practice it is not always possible to follow the recommendations, and I think that in this situation to resign from a repeat FNAC was a correct decision.
-
This case illustrates the systematic need for a new way of thinking: in contrast with the current protocol, the role of ultrasound should not be only the selection of nodules for cytology but must have play a role even in the final diagnosis.
-
The tumor presents invasive margins. Firstly, quite distant from the core of the tumor displaying numerous microcalcifications, scattered numbers of microcalcifications can be observed, which suggests the spread of the tumor. Secondly, the borders of the primary core are undefined.
-
The tumor has lobulated margins, as well.