
|
|
Chronic lymphocytic thyroiditis - Case 22.
|
|




Clinical presentation: a 42-year-old man was sent for aspiration cytology. The patient was discovered to have hypothyroidism and a multinodular goiter.
Palpation: both thyroids were firm. There was a large nodule in the left lobe.
Functional state: hypothyroidism (TSH 12.7 mIU/L).
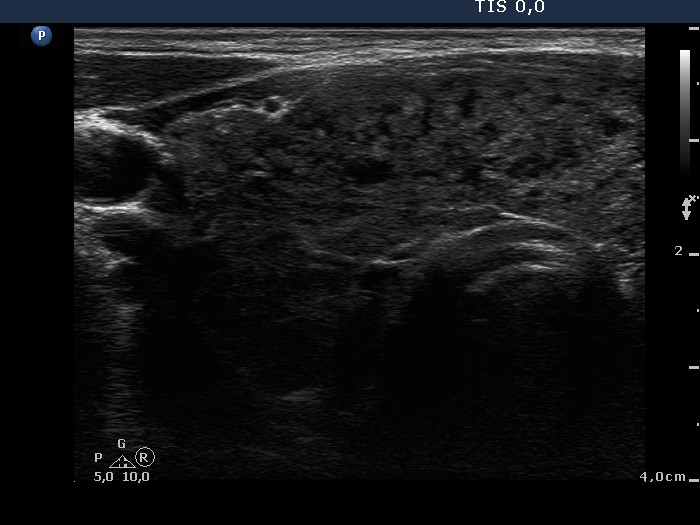
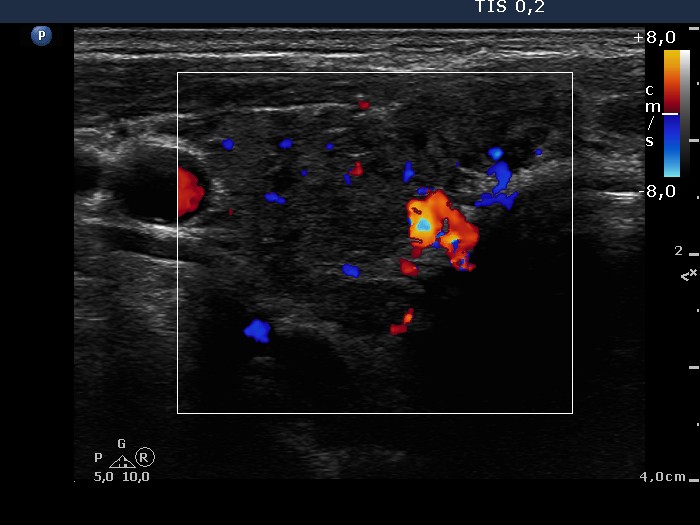
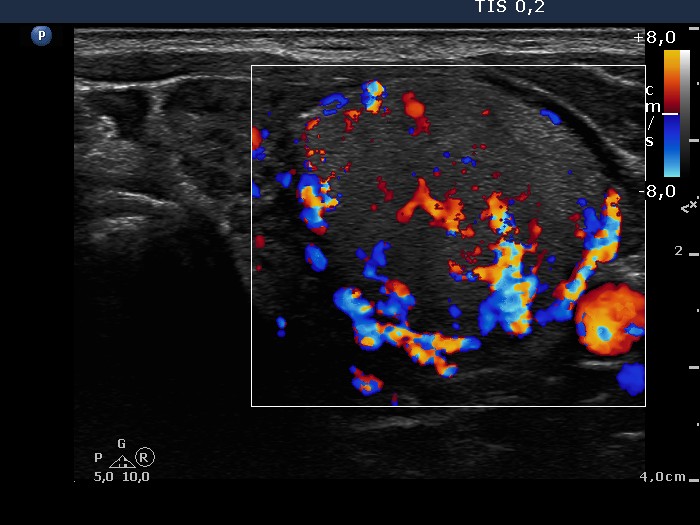
Ultrasonography: the upper part of the right thyroid presented the so-called micronodular form of Hashimoto's thyroiditis, while there were two larger hypoechogenic, nodule-like lesions in the lower part. There was a large hyperechogenic nodule presenting a halo sign and perinodular blood flow in the hypoechogenic left lobe.
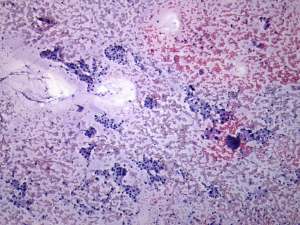
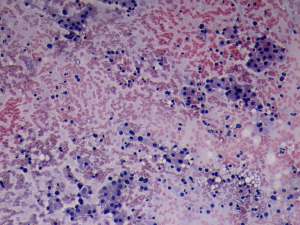
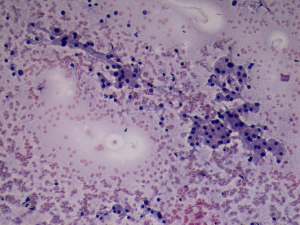
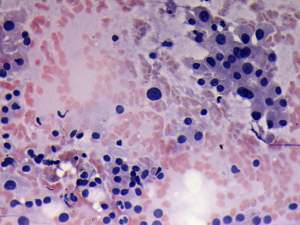
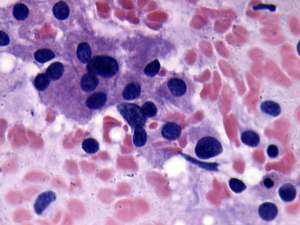
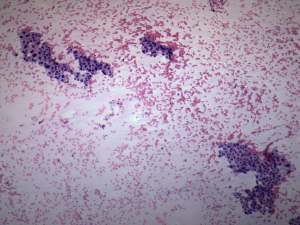
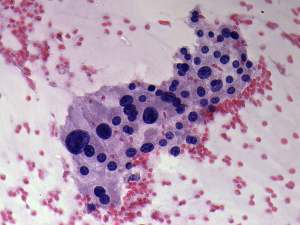
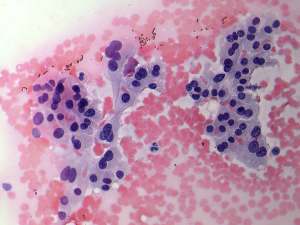
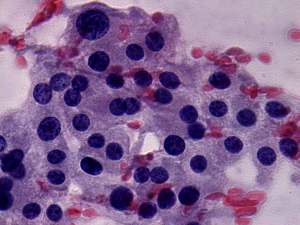
Cytology: was performed from the hypoechogenic lesion in the right lobe (first row of the cytological pictures) and from the hyperechogenic nodule in the left thyroid (second row of the cytological images). Hashimoto's thyroiditis was diagnosed in the former, while taking the sonographic pattern into account Hürthle-cell tumor in the latter case.
Histopathology: disclosed Hashimoto's thyroiditis and Hürthle-cell adenoma in the left lobe. There wasn't any nodule in the right lobe.
Comments:
-
Histopathology disclosed no nodule according to the hypoechogenic lesions in the right lobe - this is the most important lesson in this case.
-
The ratio of lymphocytes to follicular cells may vary from zero to 99.9%. In this case it was close to the former even on the smear gained from the focus of lymphocytic thyroiditis.
-
Histopathology disclosed oxyphilic tumor in the left lobe. Nevertheless, the cytological picture itself was not fully diagnostic. The lack of prominent nucleoli and the lack of tendency to dissociate cells from compact clusters stood against the possibility of a tumor.
- The combination of ultrasonography and cytology led to the correct diagnosis in the case of the Hürthle-cell adenoma.