
|
|
Ethanol sclerotherapy: toxic nodules - Case 2 |
|

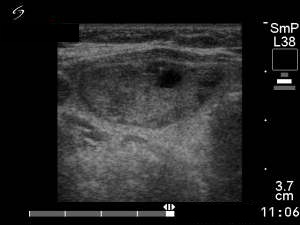























Four months before the sclerotherapy (first row of images):
Clinical presentation: a 45-year-old woman with an autonomously functioning adenoma known for 3 years was referred for evaluation. Her TSH level decreased continuously but was normal until the last checking. She had no complaints.
Palpation: a moderately firm nodule in the right lobe.
Hormonal investigation indicated euthyroidism (FT4 15.9 pM/L) with a subnormal TSH (0.19 mIU/L).
Ultrasonography: the thyroid was echonormal. There was a moderately hypoechogenic nodule in the left lobe. The lesion displayed halo sign.
Suggestion: TSH-test every six months.
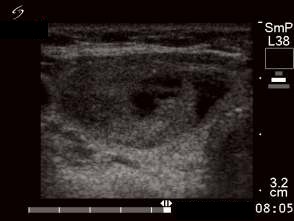
First session of the sclerotherapy (second row of images):
Clinical presentation: the patient had no complaints.
Hormonal investigation indicated subclinical hyperthyroidism (TSH 0.02 mIU/L, FT4 17.4 pM/L).
Ultrasonography: the nodule in the right lobe significantly increased.
Suggestion: definitive therapy. The patient chose ethanol sclerotherapy.
Five sessions of ethanol was administered. We gave 13 mL ethanol in all.
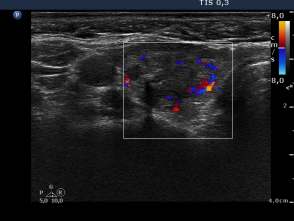
6 weeks after the last session (third row of images):
Clinical presentation: the patient had no complaints.
Hormonal investigation indicated euthyroidism (TSH 0.47 mIU/L, FT4 13.1 pM/L).
Ultrasonography: the nodule decreased significantly and became inhomogeneous.
8 years after the sclerotherapy (fourth row of images):
Clinical presentation: the patient underwent regular follow-up examinations with yearly TSH and ultrasound examinations. The size of the nodule was always smaller than 50% of the original, pretreatment volume and the TSH was in the normal range.
Hormonal investigation indicated euthyroidism ( FT4 15.2 pM/L) with subnormal TSH (0.22 mIU/L).
Ultrasonography. The size of the nodule first ever in the follow-up period exceeded the 50% of the pretreatment size, it was 55.2%.
Suggestion: to continue the follow-up.
First session of repeated sclerotherapy 11 years after the original one (fifth row of images):
Clinical presentation: the patient had no complaints. Nevertheless, she felt the nodule a bit larger.
Hormonal investigation indicated subclinical hyperthyroidism (TSH 0.02 mIU/L, FT4 16.1 pM/L).
Ultrasonography. The nodule increased further to 61% of the pretreatment volume.
We suggested radioiodine therapy but the patient wished to be treated with ethanol.
4 sessions were given, 8.6 mL ethanol was administered in all.
One year after repeated sclerotherapy (sixth row of images):
Clinical presentation. The volume of the nodule was smaller than 50% of pretreatment volume at 6-week, 3-month and 6-month follow-up as well, while the TSH was in the normal range. The patient had no complaints. She felt that the nodule became smaller.
Hormonal investigation indicated euthyroidism (TSH 0.99 mIU/L).
Ultrasonography. The volume of the nodule was 29% of the pretreatment volume.
Two years after repeated sclerotherapy (seventh row of images):
Clinical presentation: the patient had no complaints.
Hormonal investigation indicated euthyroidism (TSH 2.31 mIU/L).
Ultrasonography: the actual volume was 25% of the pretreatment. The nodule became more inhomogeneous and presented cystic areas.
Suggestion: yearly follow-up examinations.
Comments:
-
Nowadays, we do not perform sclerotherapy in autonomously functioning adenoma except for special circumstances.
-
The rate of 10-year complete success, which means that the volume is below 50% of the pretreatment and the TSH is normal, is around 60% in our patients. This figure decreases over time.