
|
|
Chronic lymphocytic thyroiditis - Case 69.
|
|


Clinical presentation: a 34-year-old woman was referred for a follow-up examination because of autoimmune thyroiditis and a nodule-like lesion discovered 5 years earlier in the post partum period. Aspiration cytology resulted in Hashimoto's thyroiditis. We advised surgery because of the size of the lesion and of the sonographic pattern. On the other hand, taking the family background into consideration, we advised yearly follow-up until she could undergo surgery. She had no complaints.
Palpation: a firm lump was palpable in the isthmic part of the right lobe.
Hormonal investigation: indicated subclinical hypothyroidism with TSH-level 5.25 mIU/L, and FT4 11.9 pM/L.
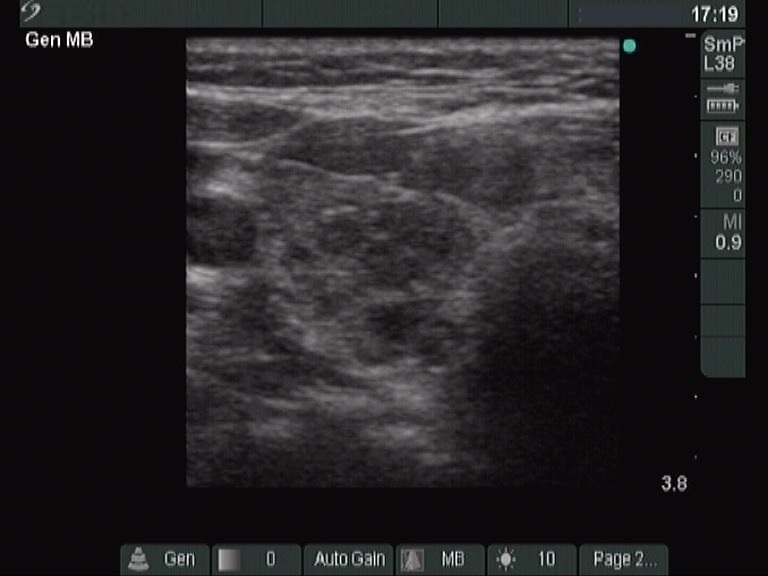
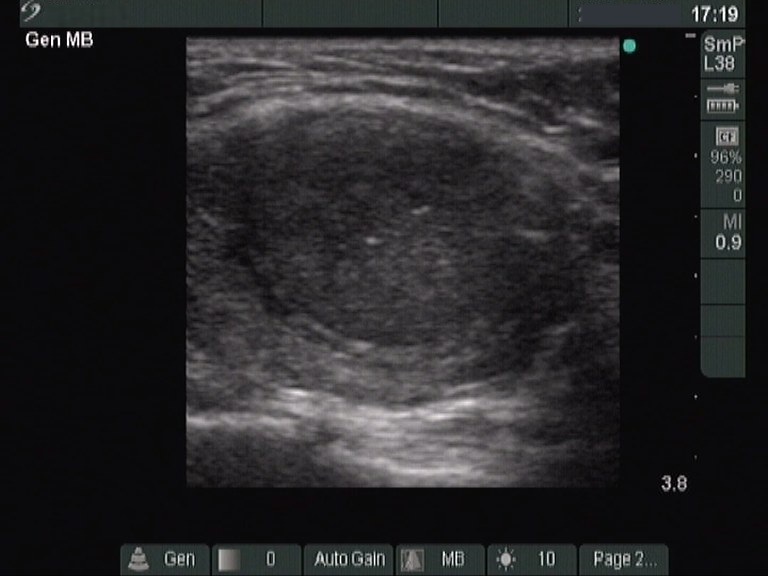
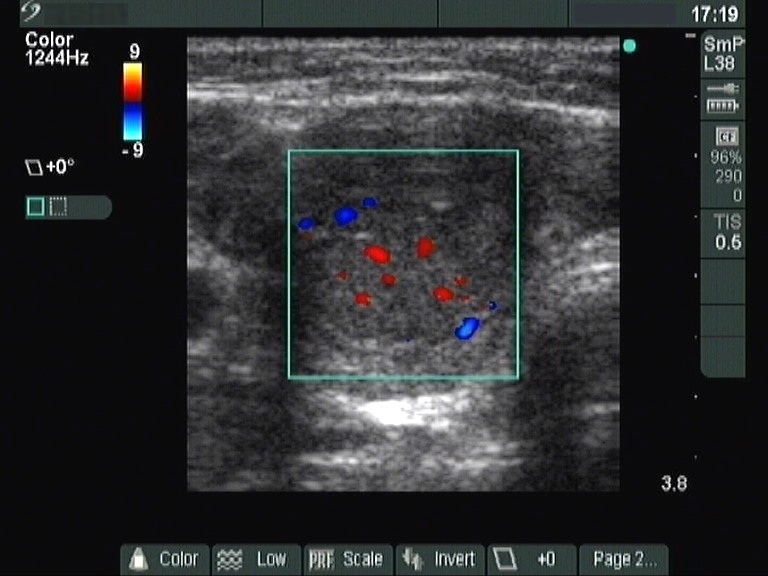
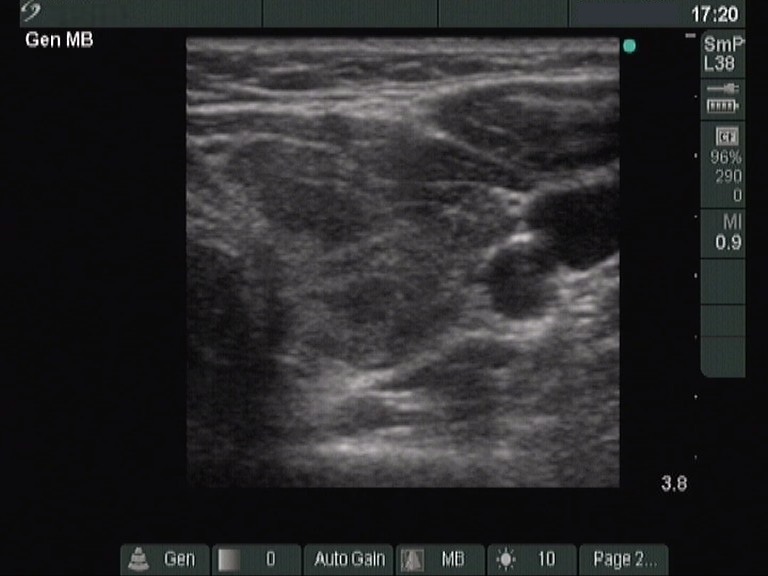
Ultrasonography: the thyroid contained around 50% hypoechogenic lesions. There was a nodule in the isthmic part of the right lobe. It contained microcalcifications and presented increased intranodular blood flow. The nodule did not change in size over the 5 years of follow-up investigations.
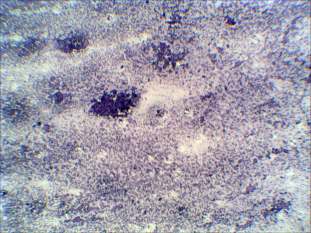
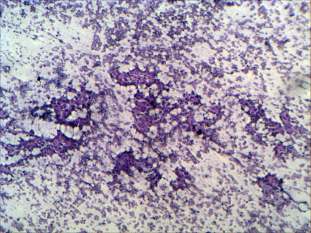
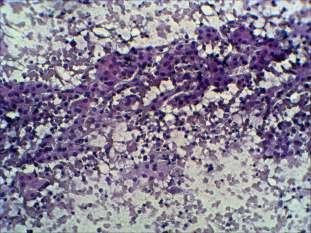
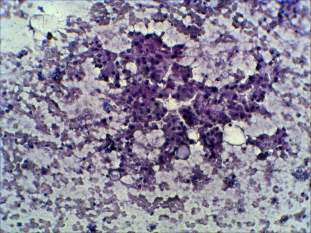
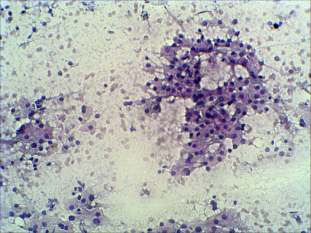
Cytological picture: oxyphilic cells predominated the smear in heterogeneous lymphoid background. They had prominent nucleoli, several atypical enlarged cells were also present. The very small number of dissociated cells, the presence of nuclear debris and lymphocytes stood against the possibility of tumor, but neoplasm could not be excluded in the cytological picture.
Cytological diagnosis: benign Hashimoto's thyroiditis.
Histopathology: benign Hashimoto's thyroiditis without any nodule.
Comment: Hashimoto's thyroiditis may imitate most thyroid disorders. Even in the presence of a nodule on palpation and ultrasound we cannot be absolutely sure that the patient has in fact a nodule. Lobules or group of lobules close to each other may imitate the presence of a true nodule. Nevertheless, this case study presents a rare situation: such US pattern means with great, however, not all probability that the patient had a nodule.