
|
|
Chronic lymphocytic thyroiditis - Case 20.
|
|






Clinical presentation: a 37-year-old man was referred for an evaluation of a 'lump in the throat' feeling.
Functional state: subclinical hypothyroidism with TSH 5.01 mIU/L, FT4 13.6 pM/L.
Palpation: the left lobe was suspicious containing a small nodule.
Ultrasonography: the thyroids were moderately hypoechogenic and displayed fibrosis. There was a relatively larger hypoechogenic lesion in the central part, and other smaller ones in the dorsal part of the left lobe. The vascularization was not specific.
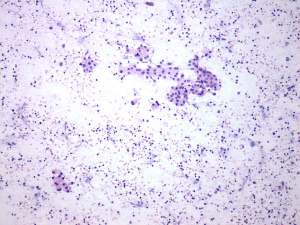
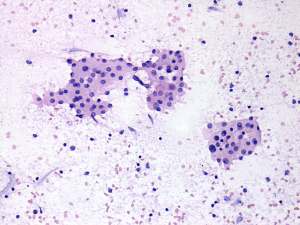
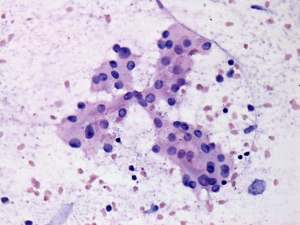
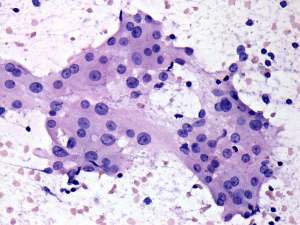
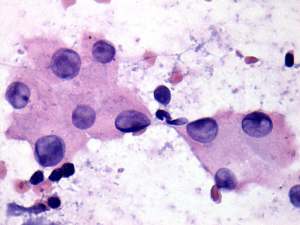
Aspiration cytology: resulted in Hashimoto's thyroiditis. Atypia of unknown significance; the possibility of a Hürthle-cell tumor cannot be excluded.
We told the patient that the risk of malignancy is around 5%. We offered a follow-up examination instead of a surgery. He decided to undergo the operation.
Histopathology: disclosed Hashimoto's thyroiditis. No nodules were found on a histopathological examination.
Comments:
-
We could not decide on utrasound whether the lesion in the left lobe would be a nodule in a pathological sense. The presence of other similar areas decreased the possibility being the larger lesion a true nodule.
-
Regarding the cytological pattern, there is no doubt that the patient has lymphocytic thyroiditis. The presence of both prominent nucleoli, grooves and inclusions raised the possibility of a Hürthle-cell tumor.