
|
|
Other rare thyroid tumors and non-thyroidal lesions in the region of the thyroid - Case 6.Adenoid cystic carcinoma of the thyroid
|
|









Clinical data: a 83-year-old man was referred for an evaluation of a newly discovered nodule in the thyroid detected on CT scan. He was operated on squamous cell lung cancer 4 years earlier. On evaluation of hoarseness lasting for 2 years, palsy of the recurrent nerve was diagnosed. CT scan did not reveal any abnormality in the thorax. Aspiration cytology performed in another hospital resulted in anaplastic thyroid cancer.
Palpation: no abnormality.
Functional state: euthyroidism (TSH-level 1.77 mIU/L).
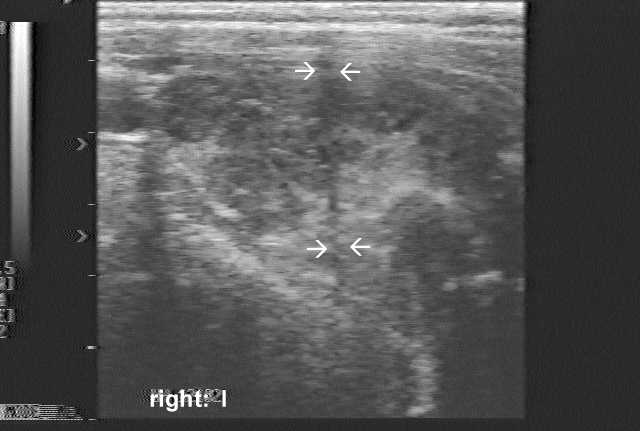
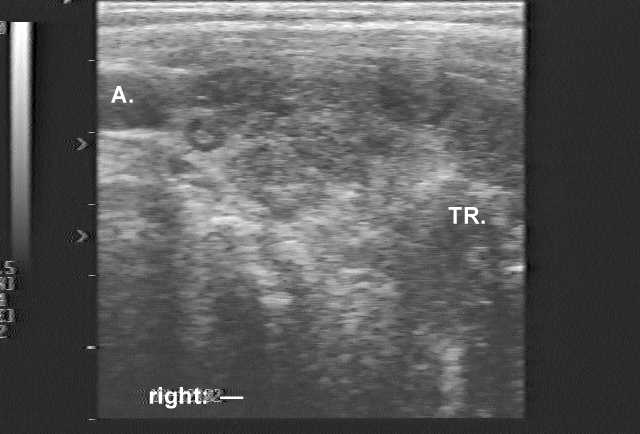
Ultrasonography: there was a hypoechogenic nodule in the dorsal part of the right lobe. The borders of the lesion were irregular. The intranodular blood flow was increased.
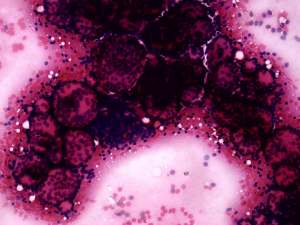
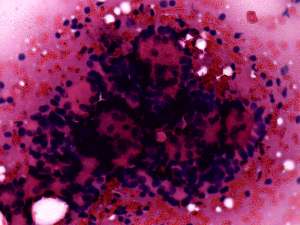
Preliminary cytological diagnosis: suspicion of carcinoma. Poorly differentiated cancer or metastasis.
Wash-out technique: normal thyroglobulin level of the remnant.
Serum calcitonin level: in normal value.
Combined diagnosis: primary thyroid cancer with great probability. The possibility of anaplastic cancer can be excluded on clinical and sonographic appearance.
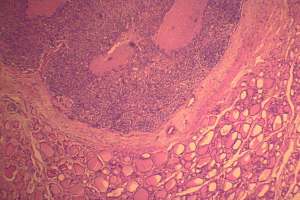
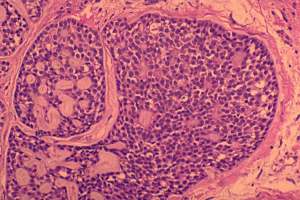
Histopathology: Adenoid cystic carcinoma of the thyroid.
Comments:
-
Anaplastic thyroid cancer is the most malignant thyroid tumor. The clinical and sonographic presentation, i.e. the 2 year history of recurrent nerve palsy and the size of the lesion excluded this type of tumor with almost 100% probability.
-
The cytological picture does not fit a common thyroid malignancy. Althought medullary cancer may present in very diverse forms, the normal calcitonin level excluded this possibility.
-
The usefulness of wash-out technique is under investigation. But normal thyroglobulin level in a metastatic tumor is more than unlikely.
-
The cytological diagnosis of insular cancer is problematic due to its rarity and lack of experience.