
|
|
Graves' disease - Case 20.
|
|

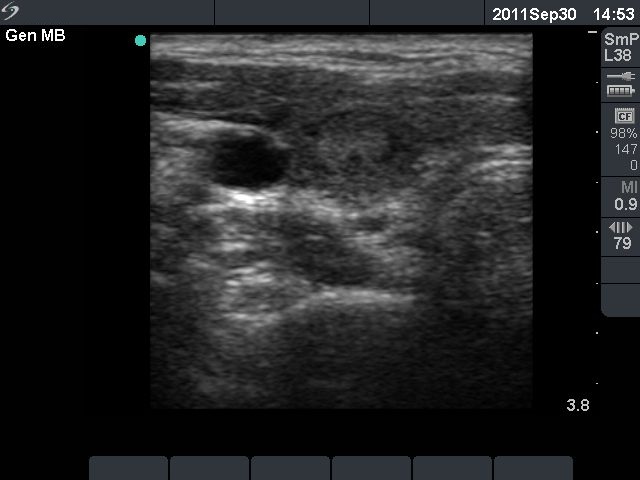
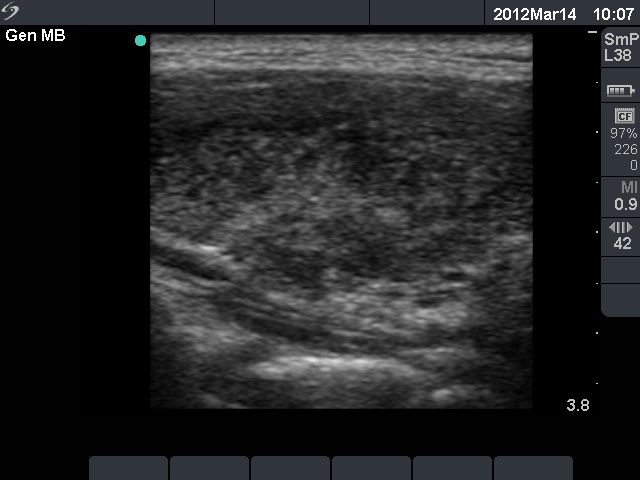


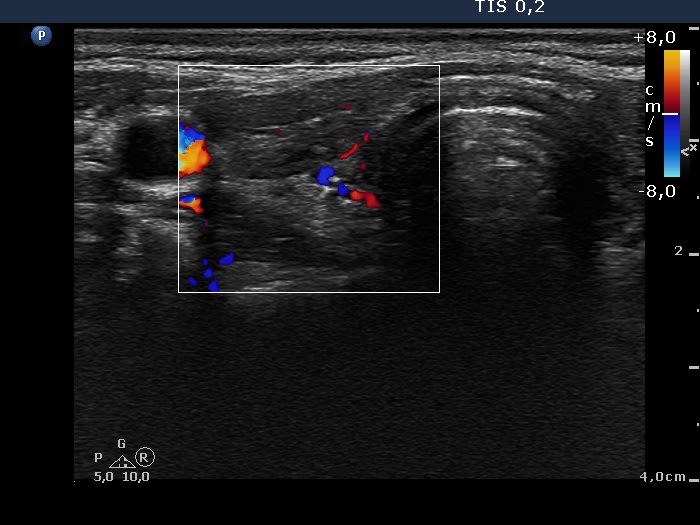


First examination (first row):
Clinical presentation: a 17-year-old girl who has been treated for hyperthyroidism for 2 years. She had no complaints.
Palpation: no abnormality.
Functional state: euthyroidism on daily 10 mg methimazole with TSH 2.14 mIU/L, FT4 13.2 pM/L.
Ultrasonography: the thyroid was echonormal with a hyperechogenic lesion in the central part of the right lobe. The vascularization was a little bit increased.Suggestion: discontinuation of thyrostatic therapy and follow-up examination 6 months later.
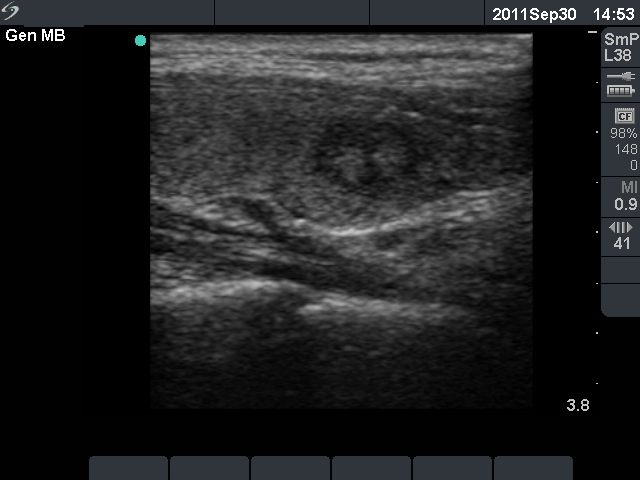
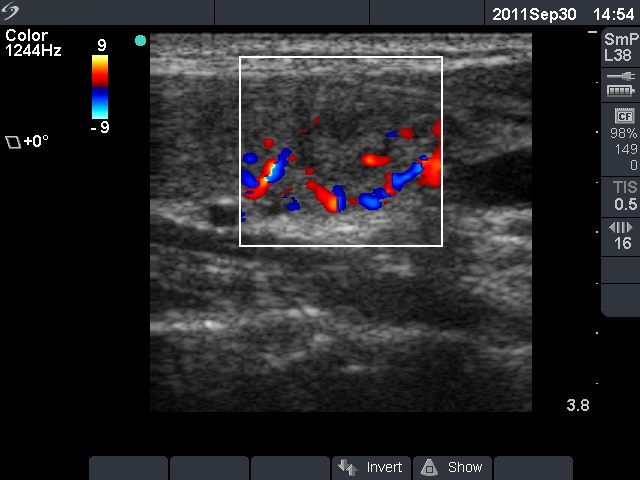
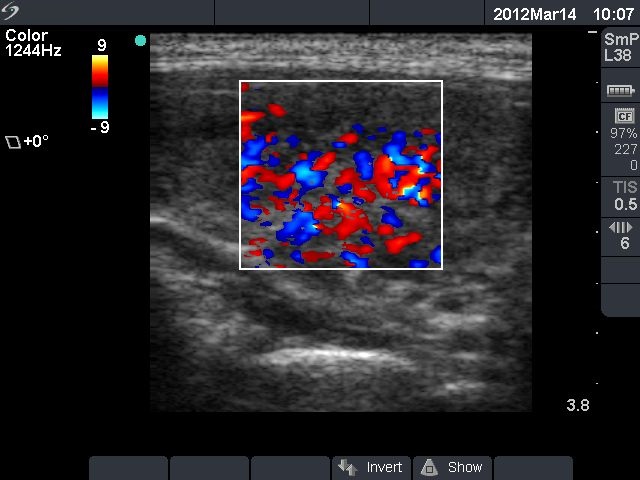
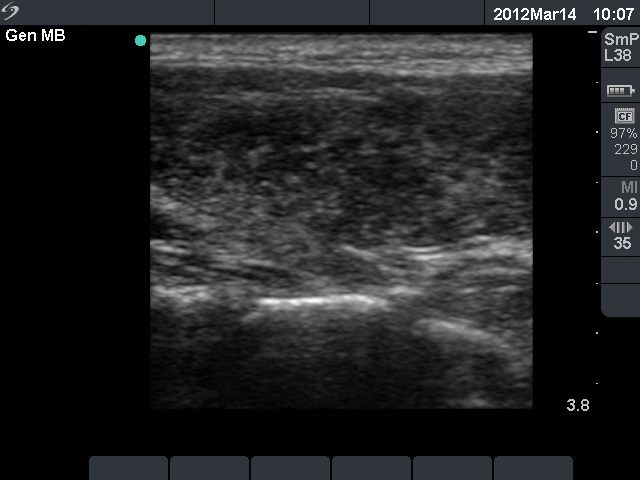
Six months after initial investigation (second row):
Clinical presentation: she had no complaints till the last several week, then she noticed increase in heart rate and fatigue.
Palpation: both thyroids were enlarged.
Functional state: hyperthyroidism with TSH-level 0.09 mIU/L, FT4 28.2 pM/L, FT3 12.8 pM/L.
Ultrasonography: the thyroids were hypoechogenic and presented increased vascularization.
Clinical diagnosis: recurrent hyperthyroidism caused by Graves's disease. We administered daily 20 mg methimazole. 2 months later when FT4 level has normalized the patient underwent radioiodine therapy.
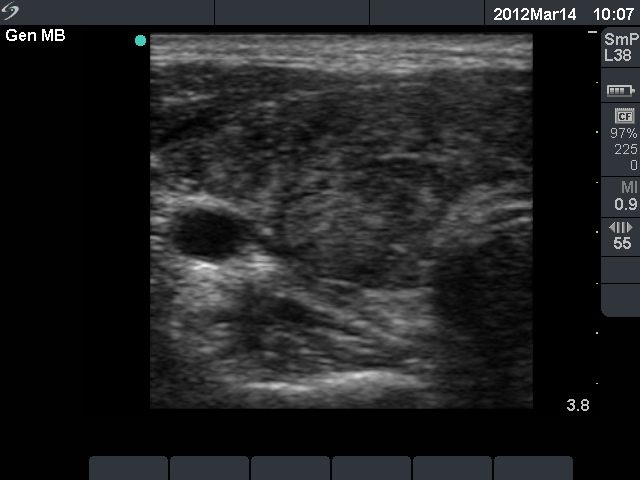
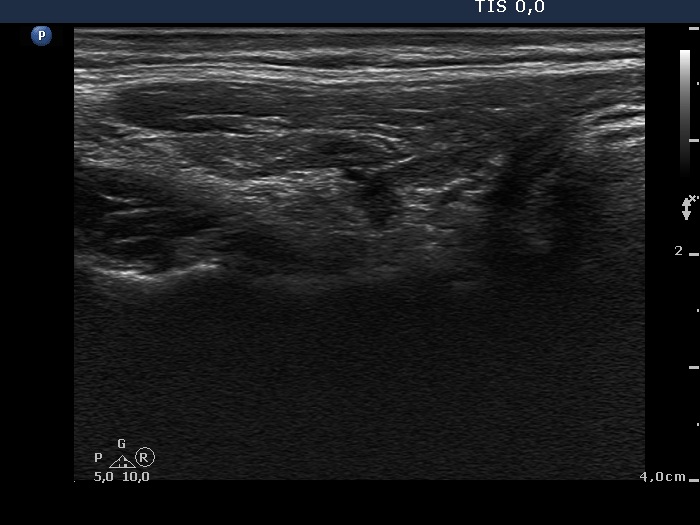
One year after radioiodine therapy (third row):
Clinical presentation: the patient had no complaints.
Palpation: the thyroid could not be palpated.
Functional state: mild hypothyroidism on daily 112.5 microgram levo-tiroxine (TSH-level 5.11 mIU/L).
Ultrasonography: the thyroids were hypoechogenic and presented extensive fibrosis. The size of the lobes decreased significantly. The thyroid presented no and decreased vascularization, right and left lobe, respectively.
Suggestion to increase the dose of levo-tiroxine to daily 125 microgram.