
|
|
Subacute granulomatous de Quervain's thyroiditis - Case 9. |
|




































Initial examination (first row of images):
Clinical presentation: a 29-year-old woman requested a second opinion. She was in the 11th week of her pregnancy. She had mild neck discomfort for 2 months. A suspicious nodule was found in the left lobe on the evaluation. Aspiration cytology was repeatedly non-diagnostic. She was told that she had thyroid carcinoma with great probability. Her endocrinologist recommended to abort the child and then to undergo thyroidectomy.
Palpation: the left thyroid was hard on palpation, but not painful.
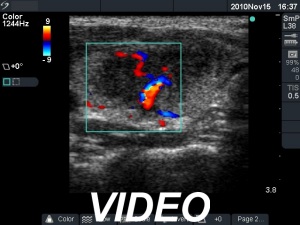
Ultrasonography: the right thyroid was echonormal and contained several small, insignificant lesions. There was a hypoechogenic lesion with blurred borders in the central and in the ventro-medial part of the left thyroid with increased intranodular blood flow.
Aspiration cytology: resulted in thyroiditis, not otherwise specified.
Laboratory tests: subclinical hyperthyroidism. Serum-calcitonin, anti-TPO, anti-hTg, TSAb resulted in normal values.
Clinical-sonographic-cytological diagnosis: subacute, de Quervain's thyroiditis.
Suggestion: regular follow-up examinations.
The details of the case history are summarized in Table.
|
Date of investigation |
Volume of hypoechogenic areas (mL) |
Pregnancy |
Therapy |
Results of laboratory investigations |
|||
|
Right lobe |
Left lobe |
ESR (mm/H) |
TSH (mU/L) |
FT4 (pM/L) |
|||
|
Initial investigation |
0.07 |
3.19 |
11th gest. week |
Nothing |
49 |
0.03 |
23.6 |
|
6 weeks after init. investig. |
0.07 |
3.38 |
16th gest. week |
Nothing |
50 |
0.06 |
13,5 |
|
3 months after init. inv. |
0.06 |
4.72 |
21th gest. week |
Starting with 50 ug l-tiroxin |
37 |
0.85 |
10.1 |
|
5 months after init. investig. |
0.08 |
0.40 |
33rd gest. week |
Continuing with replacement th. until delivery |
8 |
0.63 |
14,7 |
|
11 months after init. investig. |
7.30 |
0.18 |
4 months after delivery |
Nothing |
71 |
0.24 |
11.9 |
|
13 months after init. inv. |
6.07 |
0.21 |
6 months after delivery |
Nothing |
23 |
0.18 |
13.2 |
|
16 months after init. investig. |
0.93 |
0.24 |
9 months after delivery |
Nothing |
8 |
1.39 |
13.3 |
|
27 months after init. investig. |
0.94 |
0.21 |
20 months after delivery |
Nothing |
11 |
1.22 |
14.6 |
Comments:
-
The ultrasound pattern of de Quervain's thyroiditis and that of papillary cancer are very similar: a hypoechogenic lesion with blurred borders are found in both cases. They differ in vascularization statistically but the vascular pattern has only limited practical significance. In the acute phase of de Quervain's thyroiditis the vascularization is generally decreased but even in this case the situation was the opposite. The finding of not one but multiple hypoechogenic areas favored the possibility of subacute thyroiditis.
-
The finding of subclinical hyperthyroidism and elevated sedimentation rate were strong arguments for subacute thyroiditis.
-
We did not administer anti-inflammatory drugs because the patient was pregnant. Therefore, the hypoechogenic areas of the left thyroid decreased very slowly.
-
Although the hypothyroid state observed on 21th gestational week would normalize spontaneously, we had to administer replacement therapy because the patient was pregnant.
-
The relapse of de Quervain's thyroiditis in the contralateral lobe is a very frequent finding but not one year after the appearance of the disease. We supposed that the immunological changes during and after pregnancy explained the relatively late recurrence of the disease.
-
I do not want to comment on the suggestion of the endocrinologist who examined the patient at first. Nevertheless, even in the case of a cytologically diagnosed papillary cancer, the patient had the opportunity to put the surgical procedure on hold until her delivery.
-
I think that this case is a very good example why the thyroidologist has to do ultrasonography and then perform the ultrasound examination him- or herself. This is the only way to avoid unnecessary surgery in ambiguous cases.