
|
|
100 consecutive patients with papillary carcinoma - Case 29. |
|


















First examination - before surgery (first and second rows of images)
Clinical data: A 51-year-old woman was referred for an evaluation of neck discomfort which has been started for a year. She discovered a nodule in the isthmic part of the thyroid 5 months before the present examination.
Palpation: a firm nodule in the isthmus.
Functional state: euthyroidism (TSH 2.01 mIU/L, FT4 14,9 pM/L).
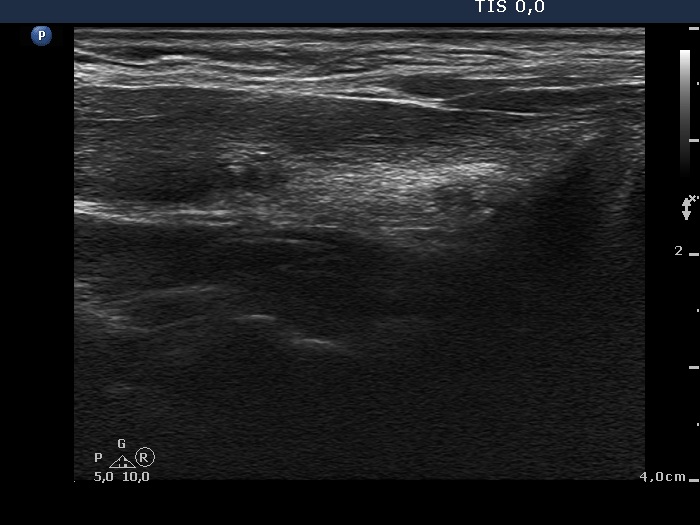
Ultrasonography: The right lobe was echonormal. There was a moderately hypoechogenic, inhomogeneous nodule with blurred borders in the left side of the isthmus. Another cystic nodule was present in the left thyroid.
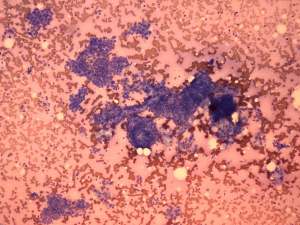
Cytological diagnosis: papillary cancer.
Total thyroidectomy was performed. Histopathology: papillary cancer based on the nodule aspirated and hyperplastic nodule based on the nodule in the left lobe. The tumor reached the capsule of the thyroid and the maximal diameter of the carcinoma was 8 mm. The tumor cells displayed significant atypia and even pleomorphism.
Four weeks after surgery (third row of images)
Clinical data: The patient visited us to get information about the further therapy and prognosis of her disease.
Ultrasonography: A moderately hypoechogenic mass composed of discrete circumscribed areas replaced the resected thyroid.
Taking the location and the morphology of the tumor into account we advised radioiodine therapy.
One year after surgery (fourth row of images)
Clinical data: The patient underwent on ablative radioiodine therapy and was well.
Palpation: no abnormality.
Functional state: subclinical hyperthyroidism on daily 175 microgram levothyroxine (TSH 0.06 mIU/L, FT4 22.1 pM/L, tireoglobulin < 0.1 ng/dL, anti-hTg 2 U/mL).
Ultrasonography: There was no thyroid parenchyma in the thyroid beds. The regenerative mass has disappeared.