
|
|
Thyroid cancers - case 727
|
|



Clinical data: A 50-year-old woman requested evaluation of a thyroid nodule. She noticed an unpleasant feeling when touching the right side of the neck.
Palpation: a firm nodule in the right lobe which was a bit tender on palpation.
Laboratory evaluation: TSH 0.94 mIU/L, aTPO below 0.25 U/mL, CRP 1.4 mg/L.
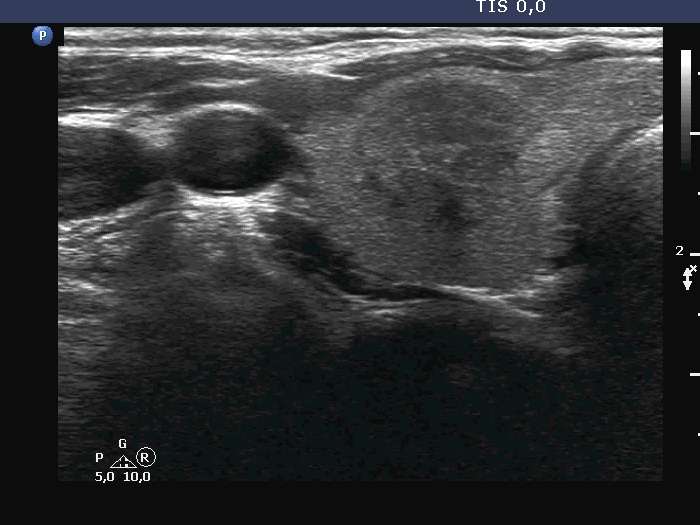
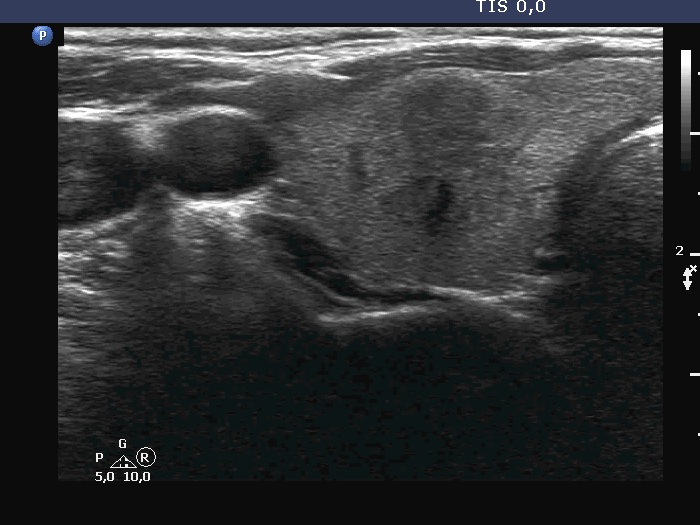
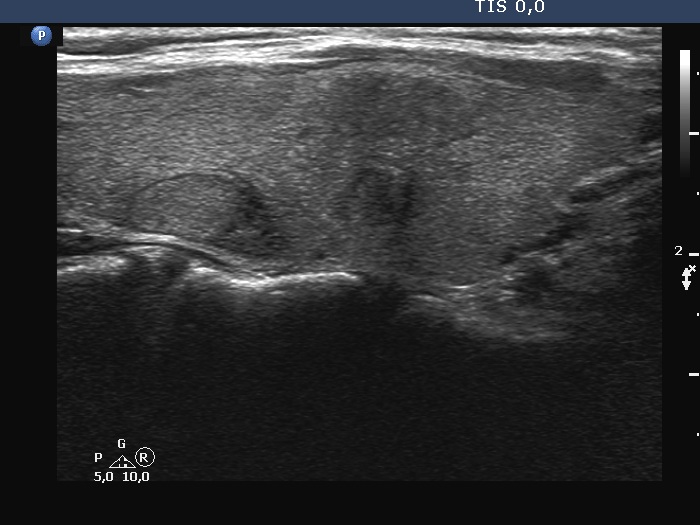
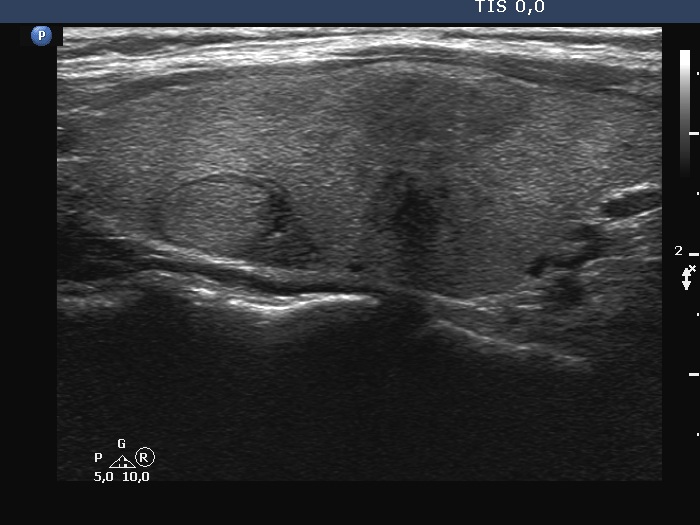
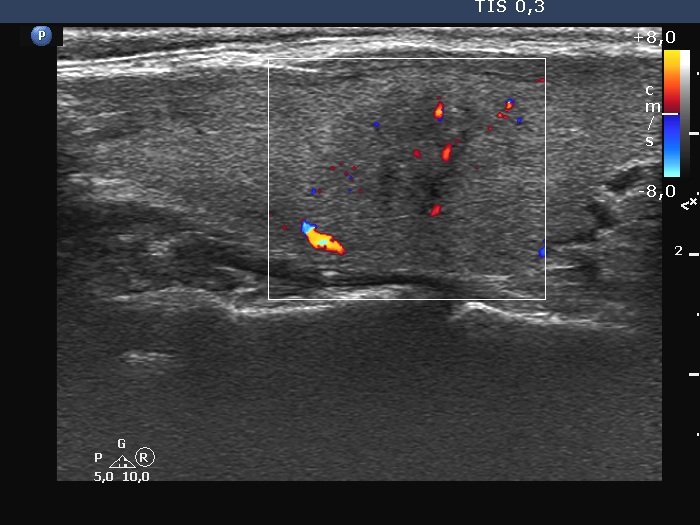
Ultrasonography. The thyroid was echonormal. There were three discrete lesions in the right lobe while several others in the left lobe. There was only one remarkable among them. This was in the ventral part of the right lobe. It was minimally hypoechoic, presented with partly irregular, partly blurred borders. Intranodular vascularity was detected.
Cytological diagnosis: of the lesion in the right lobe resulted in oxyphilic variant of papillary cancer.
Serum calcitonin resulted in 7.91 pM/L (normal value 0-5.33).
Total thyroidectomy and right lymphadenectomy were performed. Histopathology disclosed medullary cancer according to the lesion in question. There were benign hyperplastic nodules in the right lobe while no discrete lesion was found in the left lobe. None of the removed lymph nodes contained metastatic focus.
Six weeks after the surgery, serum calcitonin was 0.31 pM/L.
Comments.
-
The most common failure in the cytological diagnosis of medullary cancer is to confuse it with an oxyphil tumor. This was the 38th case of medullary cancer in my cytological practice but despite the quite a significant practice, the error occurred again. I do not perform routinely serum calcitonin test neither in all nor in hypoechoic nodules but measure calcitonin in every case of suspected oxyphilic tumors.
-
The ultrasound and clinical presentation were remarkable, subacute thyroiditis had to be considered. I only mention that the neck discomfort ceased only after the removal of the tumor.