|
Transverse scan |
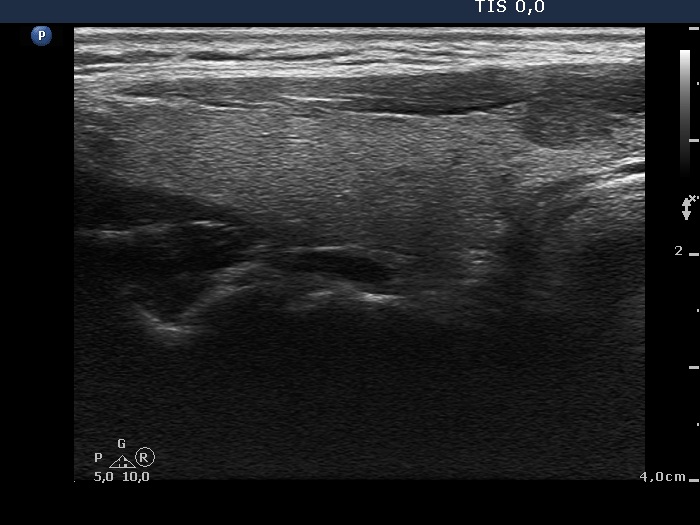
Longitudinal scan |
 |
 |
The nodule is brighter than the strap muscle while darker than the extranodular tissue and does not show any suspicious sign. This is an EU-TIRADS 4 lesion.
|
|
|
|
Transverse scan |
Longitudinal scan |
 |
 |
The nodule is a dominantly iso/hyperechoic lesion with a minimally hypoechoic minority part. According to the rules of the EU-TIRADS, this should be regarded as a TIRADS 4 nodule.
|
|
|
|
Transverse scan |
Longitudinal scan |
 |
 |
The lesion should be regarded as a TIRADS 4 nodule because the echogenicity was minimally/moderately hypoechoic and the nodule did not show any suspicious findings. The undulation at the lower-medial part of the lobe simply follows the arch of the trachea, therefore this is not a pathological form of irregular borders.
|
|
|
Transverse scan |
Longitudinal scan |
 |
 |
The nodule is a dominantly iso/hyperechoic lesion with a minimally hypoechoic minority part. According to the rules of the EU-TIRADS, this should be regarded as a TIRADS 4 nodule.
|
|
|
Benign cystic-colloid goiter (cytology) - case 2123
|
Transverse scan |
Longitudinal scan |
 |
 |
This is again a dominantly iso/hyperechoic lesion with a minimally hypoechoic minority part. According to the rules of the EU-TIRADS, this should be regarded as a TIRADS 4 nodule. The intranodular echogenic figures are related to ventral cystic areas, therefore, these should be regarded as microcalcifications. These are back wall figures caused by posterior enhancement
|
| |
|
| |
|
| |
|
| |
|
| |
| |
| |
|