|
Transverse scan |
Longitudinal scan |
 |
 |
 |
 |
The less hypoechogenic area pointed with red arrows located lateral to the main body of the tumor is suspicious being presentation of infiltration of the parenchyma. The right, longitudinal scan is more obvious: the area pointed with yellow arrows upper to the main body is caused very likely by spread of the tumor into the normal parenchyma.
|
|
|
Transverse scan |
Longitudinal scan |
 |
 |
|
 |
The main body of the tumor is pointed with red arrows, while yellow arrows point to infiltration of the parenchyma. The hallmark of these areas is the presence of microcalcifications.
|
|
|
|
Transverse scan |
Longitudinal scan |
 |
 |
 |
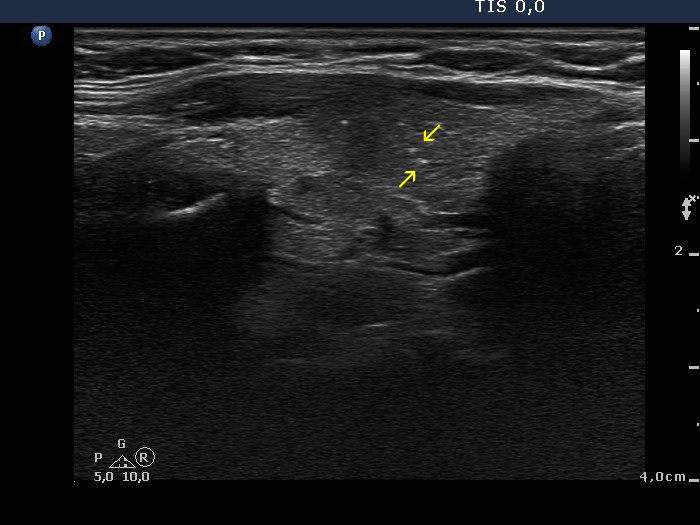 |
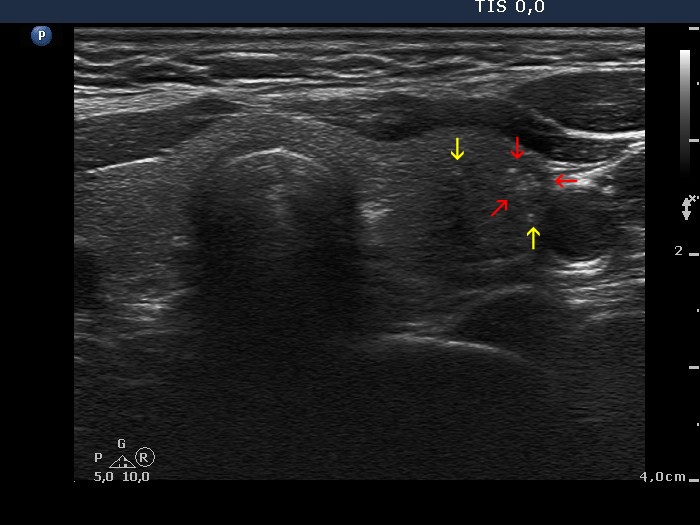
This is not a decisive but only a suspicious pattern. Lower to the main body of the tumor, there are several microcalcifications (yellow arrows). The presence of these isolated microcalcifications raises the possibility of infiltrative spread of the tumor. Although the less hypoechogenic area pointed with red arrows dorsal to the tumor might be also presentation of extrathyroidal spread, such pattern has limited if any relevance; a focus of thyroiditis might be also the cause. Be aware that the main difference between the non-specific finding in the left image and the suspicious pattern in the right image is based on the lack (left) and the presence (right) of microcalcifications. The possibility of extrathyroidal spread should be also considered: the ventral part of the nodule cannot be distinguished from the strap muscle running on the ventral surface of the lobe.
|
|
|
|
Transverse scan |
Longitudinal scan |
 |
 |
 |
 |
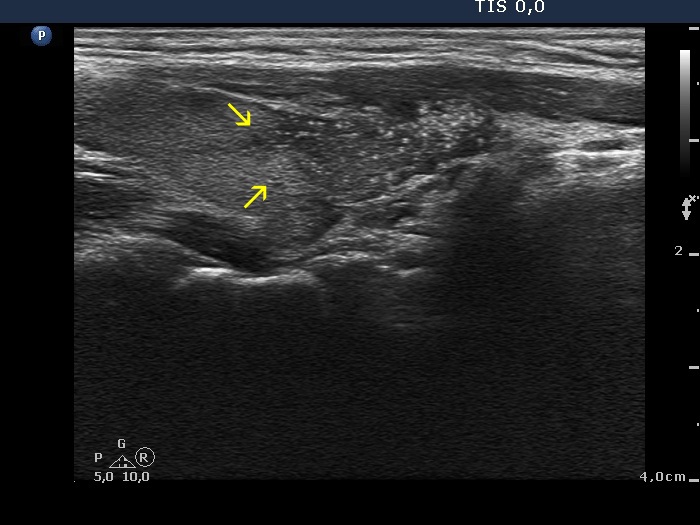
The primary tumor focus (signed with red arrows) was 4 mm in maximal diameter in histopathology. Scattered echogenic punctate granules (microcalcifications) are pointed with yellow arrow. The tumor invaded the normal parenchyma.
|
|
|
|
Right lobe longitudinal scans
|
 |
 |
 |
 |
The borders of the nodule are equivocal, yellow arrows point partly to projection of the tumor, partly to isolated microcalcification. The latter seem to be located outside the main body of the nodule.
|
|
|
|
Left lobe longitudinal scans
|
 |
 |
 |
 |
The yellow arrows point to the invasive areas of the tumor.
|
|
|
Transverse scan |
Longitudinal scan |
 |
 |
 |
 |
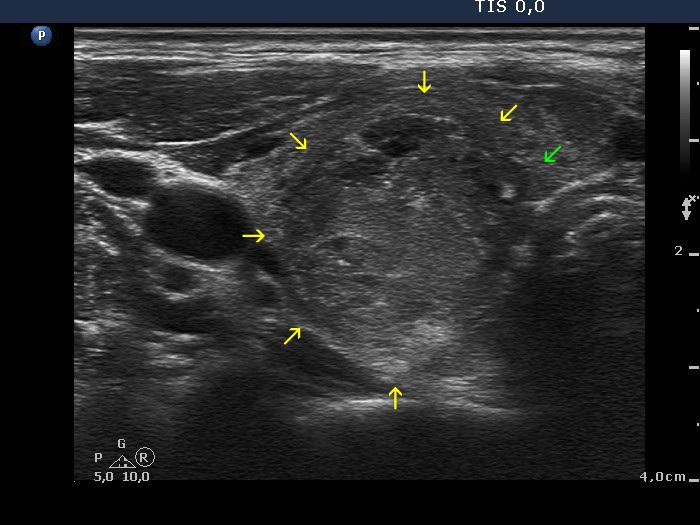
It seems to be evident that the borders of this lesion pointed with yellow arrows are irregular. On the other hand, it is difficult to group into one or another well-characterized subgroup of pathological borders. Green arrow points to a lobulated part while red arrows do to spiculated parts of the tumor.
|
|
|
Hashimoto's thyroiditis (histology) - case 2171 |
 |
 |
 |
 |
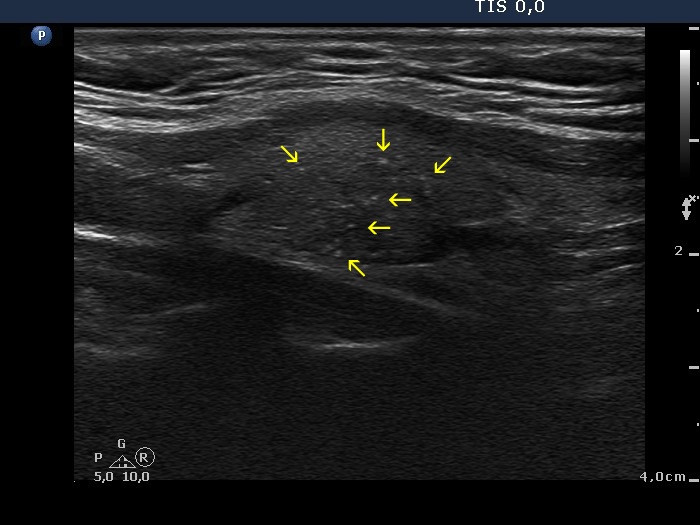
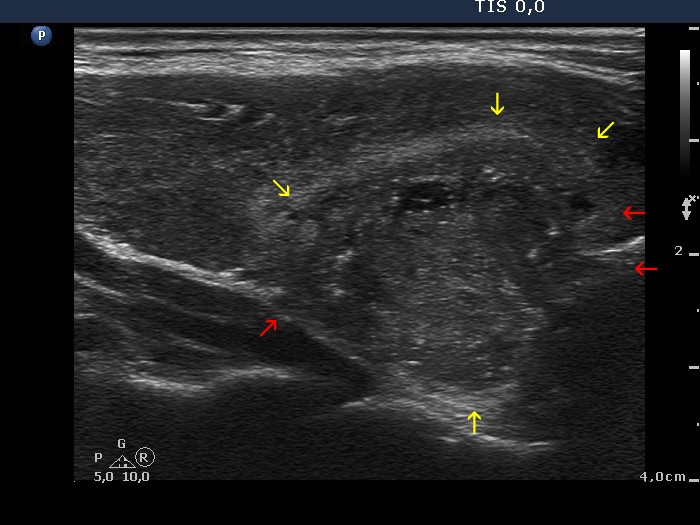
This is one of the very few cases in my practice which did not prove to be papillary cancer, although the ultrasound pattern seemed to be almost diagnostic of an invasive spread of papillary cancer. The suspicious lesion is located between red arrows. Yellow arrows point to microcalcifications located quite in a distance from this core. Note that the borders of the discrete lesion cannot be determined. This type of invasive growth does not correspond either to spiculated or to lobulated borders and is clearly different from a usual pattern of blurred borders.
|
|
|
Papillary carcinoma (histology) - case 469 |
Transverse scans |
Longitudinal scans |
 |
 |
 |
 |
The core of the tumor is marked with yellow arrows. Red arrows point to punctate echogenic foci (microcalcifications), which are located in a distance from the primary tumor.
|
|
|
|
Transverse scan |
Longitudinal scan |
 |
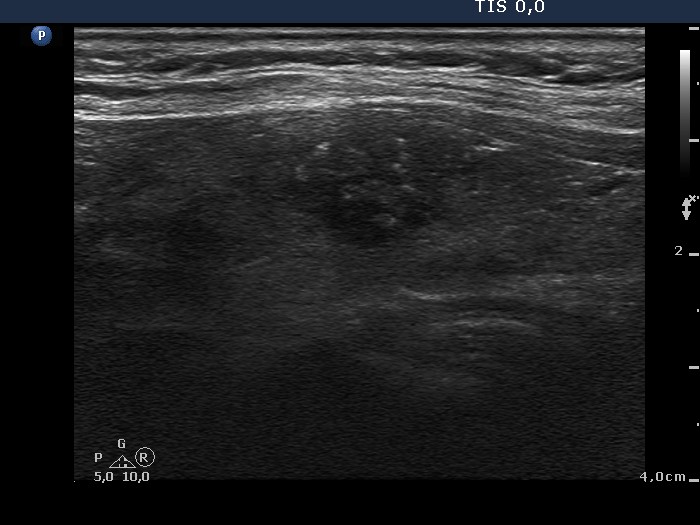 |
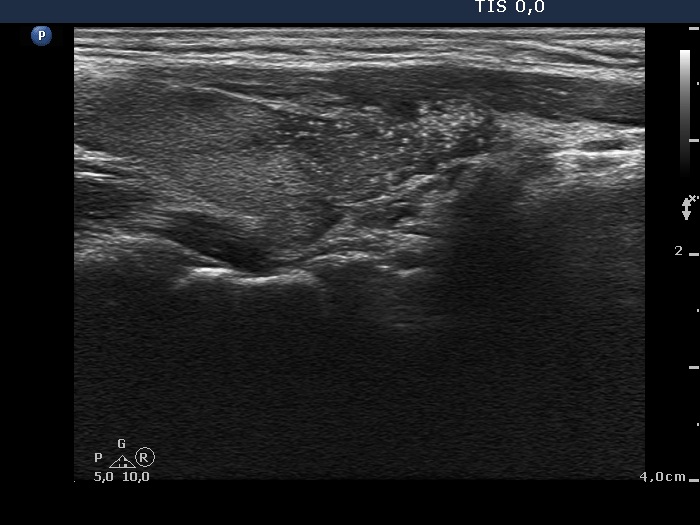
Both the tumor and the extranodular part of the lobe have echogenic figures. Most of them are less bright than a typical microcalcification, moreover they are predominantly linear. Therefore, these figures do not correspond to microcalcifications but fibrotic vessels; although the pattern resembles invasive spread, in fact, does not correspond to this subtype of non-regular margins.
|
