
|
|
The composition of the nodule - case 1792
|
|






Clinical presentation: A 48-year-old woman was operated for papillary cancer 17 years earlier. A lobectomy was performed and a T2NO tumor was found. The patient refused completion of therapy. She detected a nodule in the left thyroid 6 weeks before the present examination.
Palpation: a multinodular goiter.
Functional state: euthyroidism (TSH 1.01 mIU/L).
Ultrasonography. The right thyroid was echonormal. There were four nodules in the left lobe, two in the upper, one in the middle and one in the lower part of the lobe. The larger nodule in the upper third was a dominantly cystic nodule. The solid part was minimally hypoechoic, the lesion presented halo and signs of perinodular blood flow. Although the solid part displayed lobulation, the borders of the nodule were regular.
US-guided FNAC was performed from the solid part of the nodule in the upper part of the left thyroid.
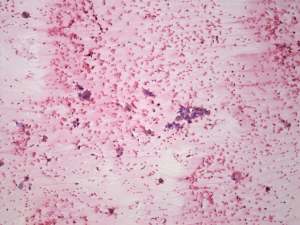
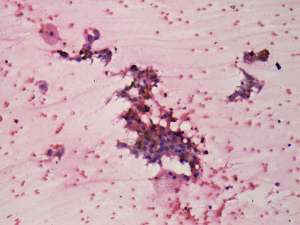
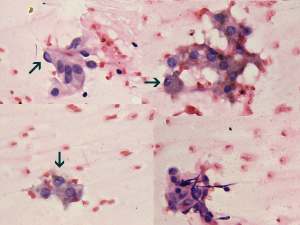
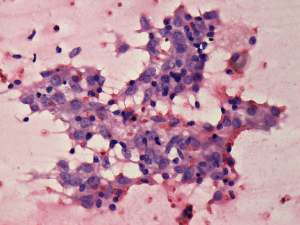
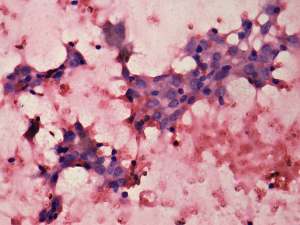
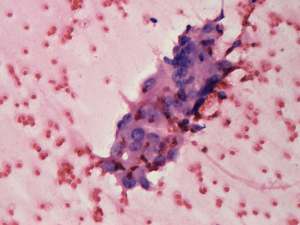
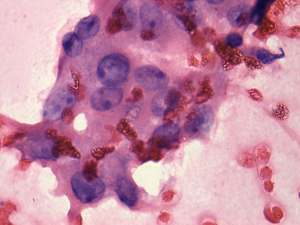
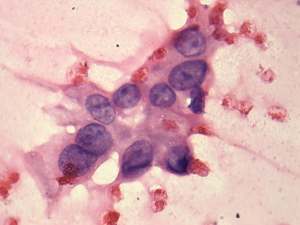
Cytological picture: There was no colloid, but many macrophages in the background. Follicular cells were arranged in non-specific groups. Occasionally nuclear crowding and overlapping could be observed. Because of the degenerative changes, the nuclear details were not unequivocal, but we have found intranuclear structures resembling grooves.
Cytological diagnosis. Suspicion of papillary carcinoma.
Histopathology. Encapsulated papillary carcinoma corresponding to the nodule in the upper part of the left lobe. The remaining nodules proved to be benign hyperplastic lesions.
Comment.
- The borders of a nodule always refer to the outer surface and not to the inner content. It means that in mixed nodules, the lobulation of the solid part should not be considered irregular.
- The malignant nodule belongs to central-type cystic lesions because tiny solid portions can be found all along the inner wall of the lesion. The nodule in the lower part is also a central-type cystic lesion.
.