
|
|
Elastography - case 2150
|
|



Clinical presentation: A 67-year-old woman came to a follow-up examination. First, I met the patient 17 years ago when a multinodular goiter has been diagnosed with a hypoechoic lesion in the left lobe with the diameters of 12x10x13 mm (width, depth, length, respectively). Cytology resulted in benign follicular proliferation.
Palpation: no abnormality.
Laboratory test: TSH 3.07 mIU/L, FT4 12.3 pM/L.
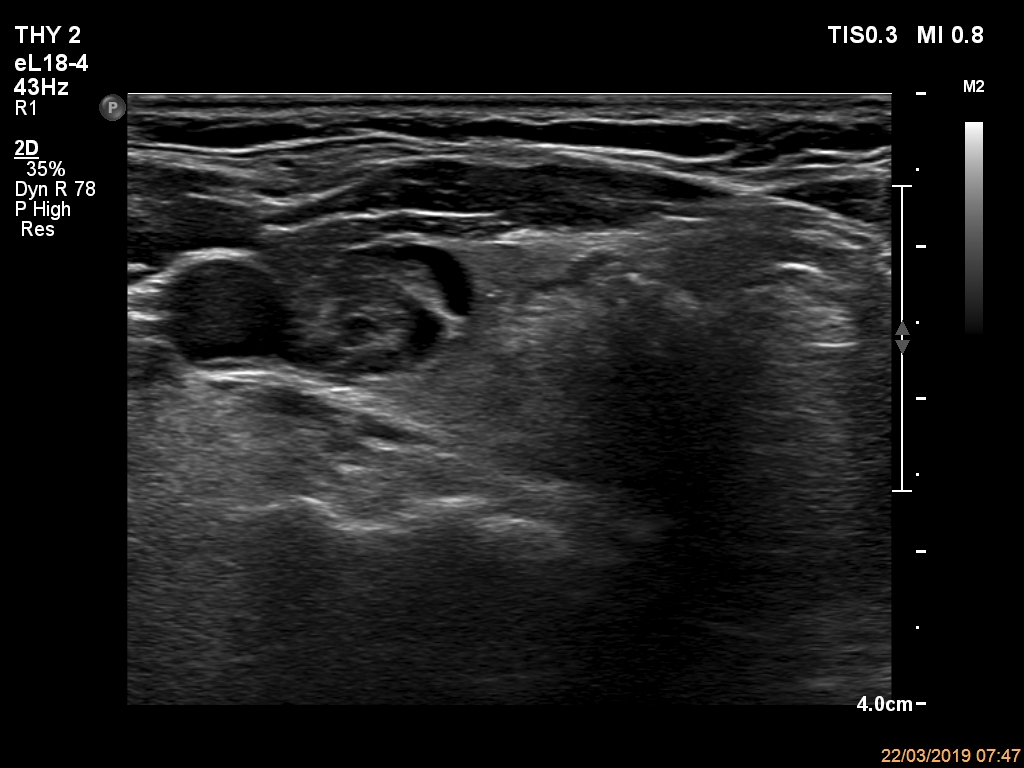
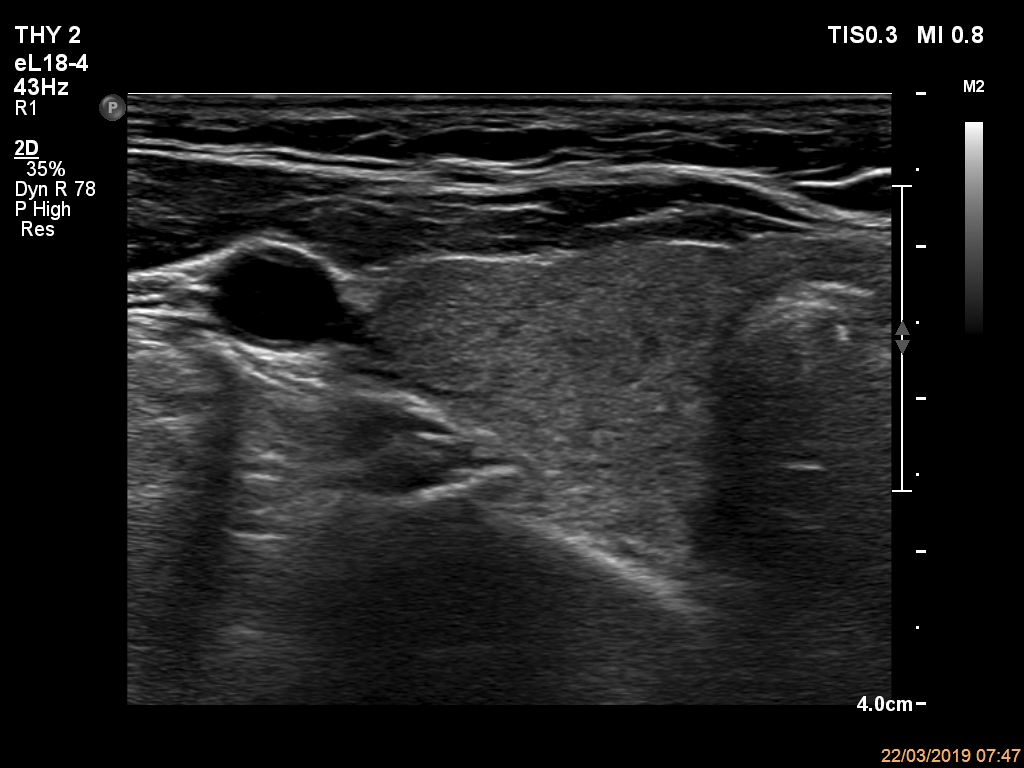
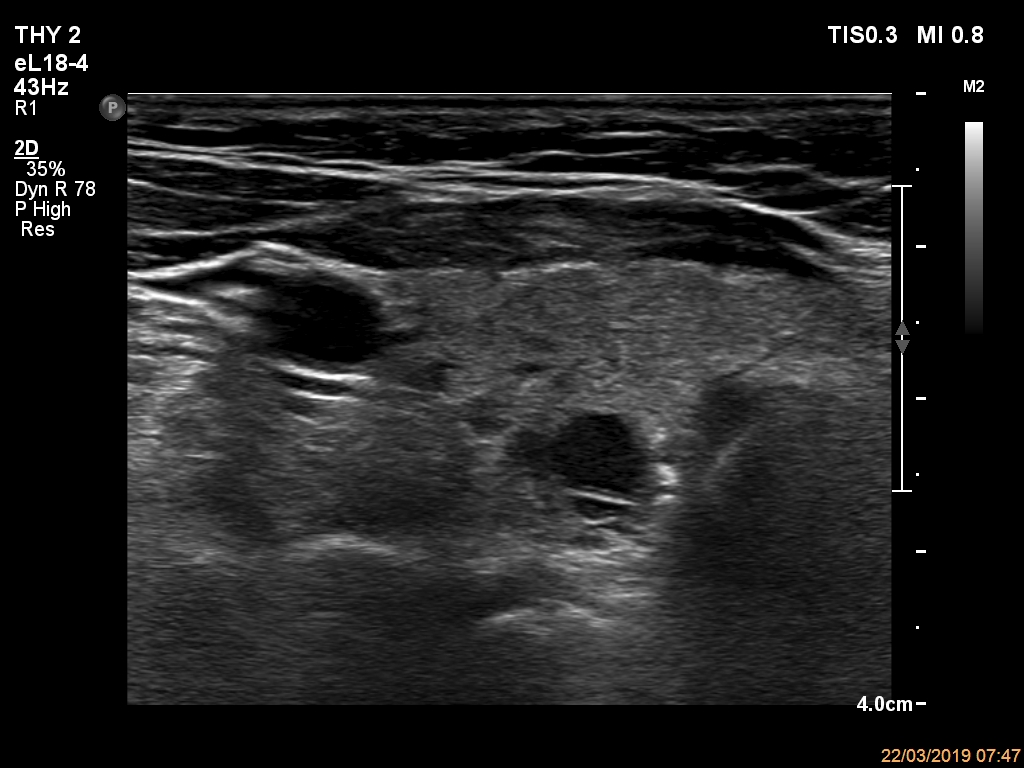
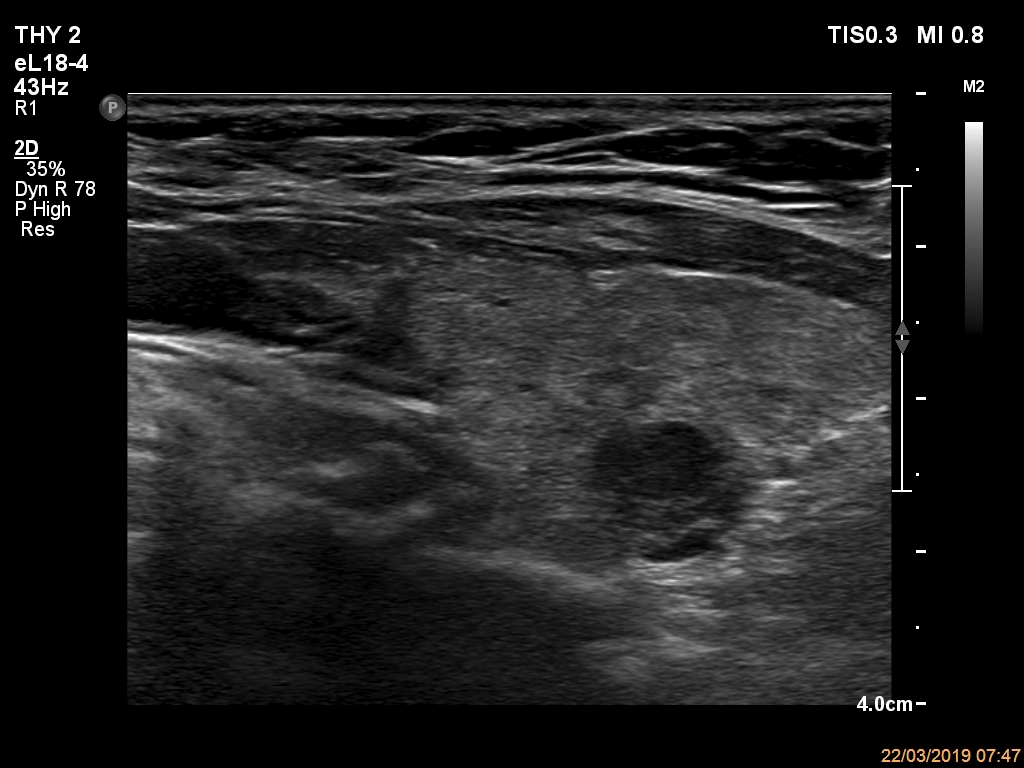
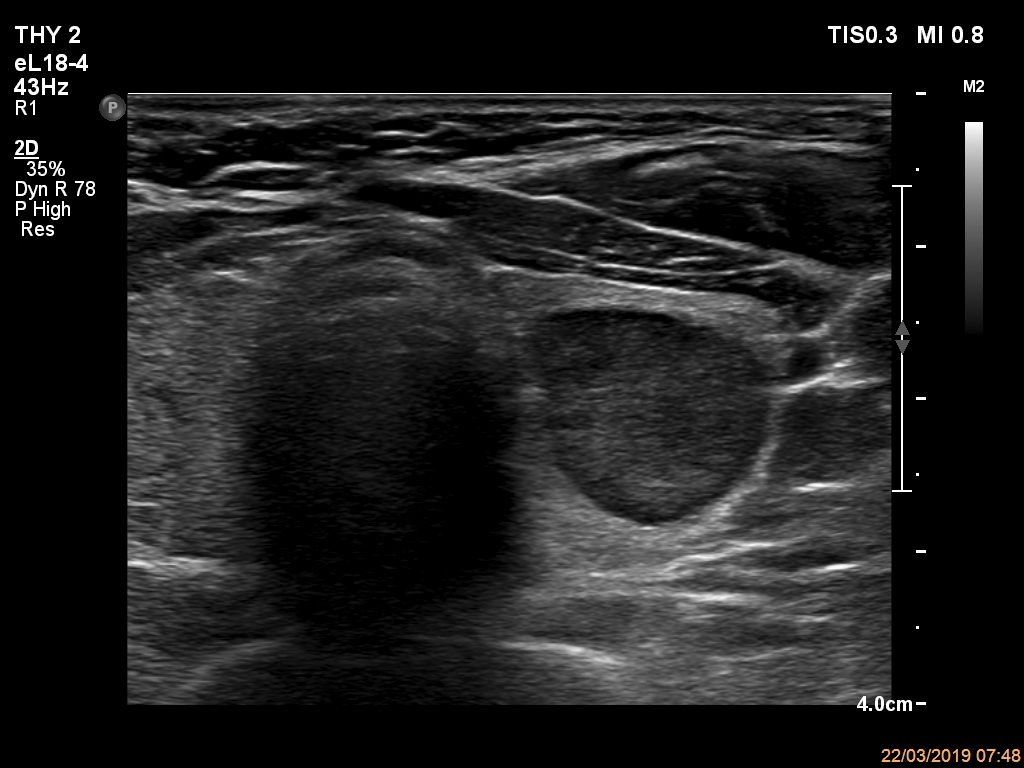
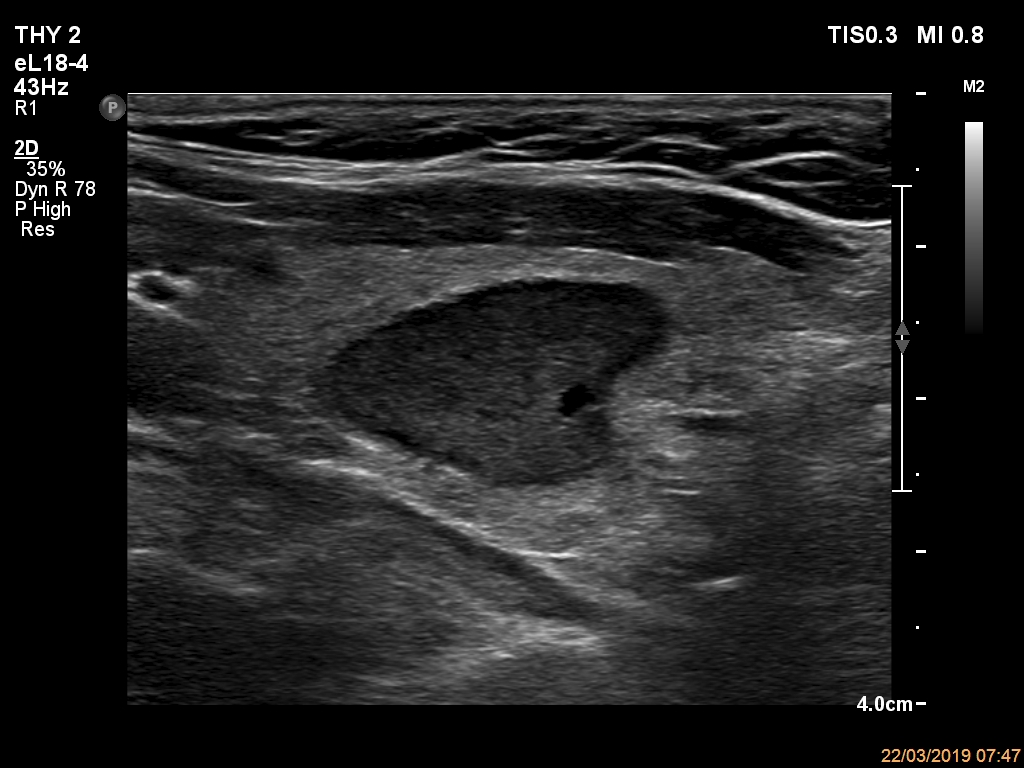
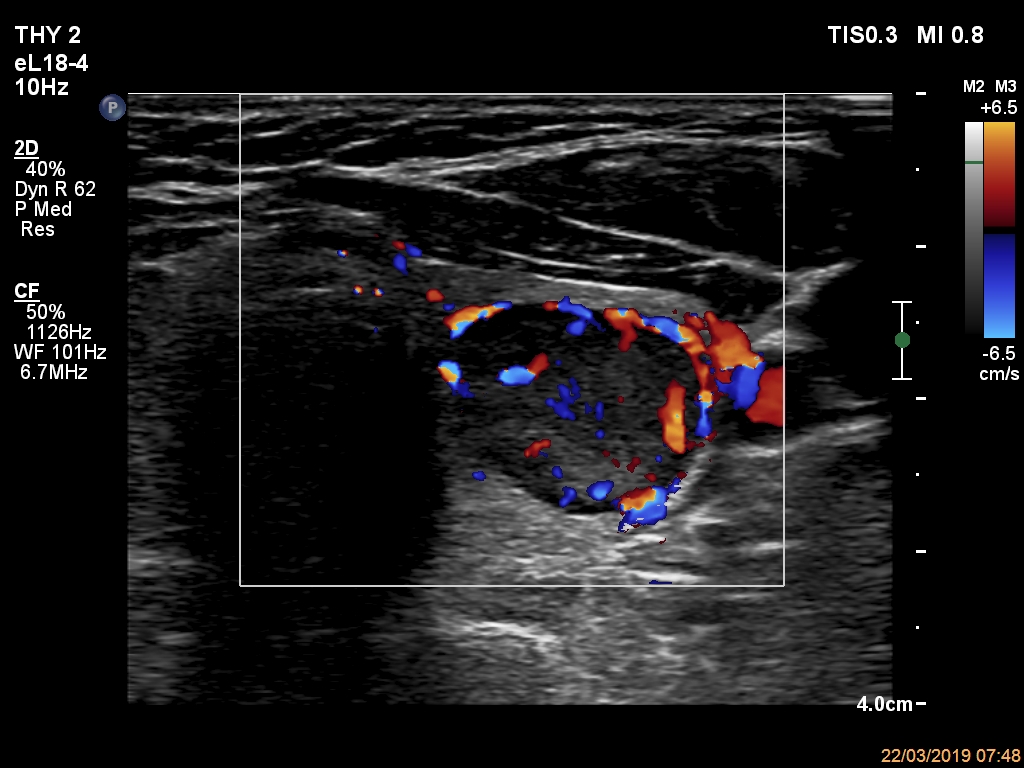
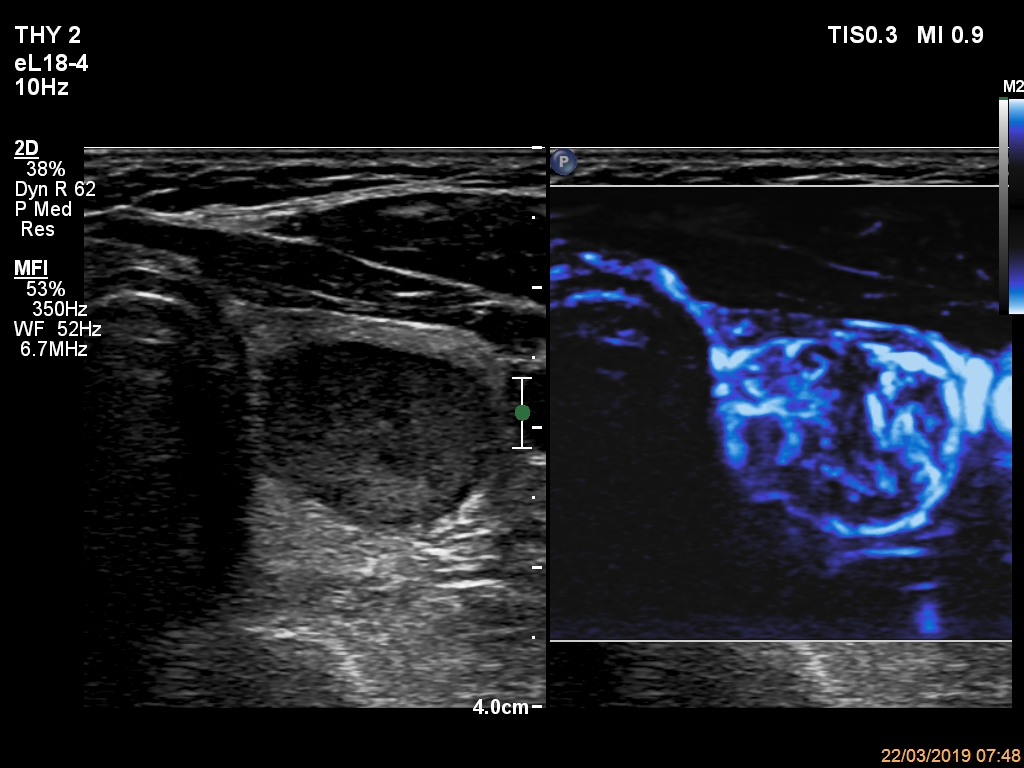
Ultrasonography. The thyroid was echonormal and had multiple nodules. The only lesion of a possible oncological importance was in the left lobe. It was hypoechoic. The dimensions were 16x14x23 mm (width, depth, length, respectively). The lower border presented an undulation which was caused by another, hyperechoic nodule. The nodule presented a predominant perinodular blood flow and had an average rigidity on elastography.
FNA resulted in follicular tumor without any significant atypia. In such events, the risk of malignancy is not greater than 2%
We discussed the possibilities with the patient and we decided on further check-up.
Comments.
-
The risk of malignancy in the event of a follicular tumor depends on many circumstances. Among these, iodine deficiency and cytological atypia are perhaps the most important. Iodine deficiency within follicular tumors increases the benign form much more than the malignant form. In contrast with the American data which show a 25-50% risk of malignancy in follicular tumors, this risk is only 3-4% in Hungary. This significant difference means that we need different approach managing follicular tumors.
-
The nodule in the left lobe illustrates non-pathological form of lobulated margins.