
|
|
TIRADS - case 2086
|
|




Clinical presentation: A 14-yr-old girl was referred for evaluation of an elevated TSH. She was investigated because of fatigue.
Palpation: no abnormality.
Laboratory tests: TSH 4.97 mIU/L, FT4 12.4 pM/L, aTPO 7 U/mL.
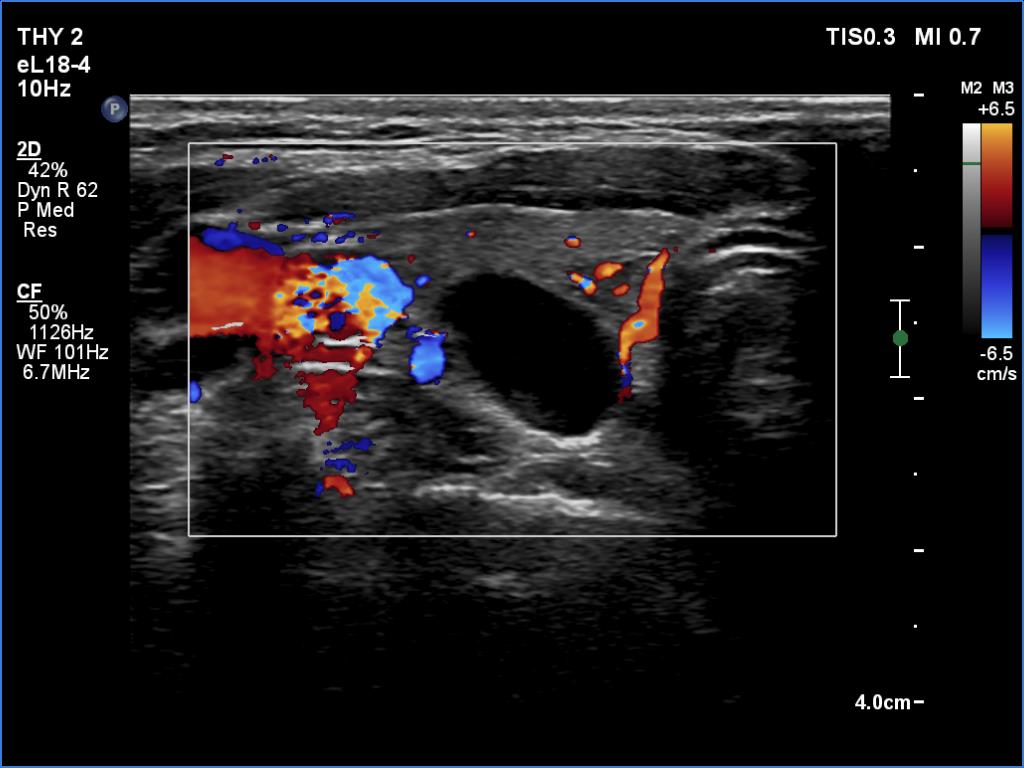
Ultrasonography. The thyroid was echonormal. There were several small hypoechoic areas in both lobes and a cystic nodule in the right lobe. At first sight the nodule seemed to be a pure cyst. However, thorough analysis revealed a tiny echonormal solid area in the dorsal part of the lesion. Therefore, this nodule does not meet the criteria of a pure cyst. The lesion presented taller-than-wide shape.
Suggestion. TSH determination in a year, ultrasound in 3 years.
Comment.
-
In incipient forms of Hashimoto's thyroiditis, the ultrasound is more sensitive than aTPO. A minimal degree of TSH elevation at this young age is not abnormal.
-
If we detect any solid part within an almost completely cystic nodule than the lesion should not describe as a pure cyst. Indeed, this cyst belongs to the peripheral-type subgroup.
-
This case illustrates one of the most important limitations of taller-than-wide shape. A nodule inevitably follows the anatomy. The cartilage of the trachea hinders the horizontal spread, therefore the only remaining route for the nodule is to extend in the perpendicular direction.
- The cystic lesion can be regarded as EU-TIRADS 2 or EU-TIRADS 3 nodule, depending on the judgement of the uncertain structure at the cystic wall. Nor can it be ruled out to classify the lesion as EU-TIRADS 5 due to the nonparallel orientation. However, it is more rational and in the best interest of the patient to classify the lesion as EU-TIRADS 2.