
|
|
Teamwork - case 1257
|
|



Clinical data. For the first time since childhood, a 41-year-old man, a mathematician, underwent a medical examination during a complex screening organized at his workplace. The only abnormality was a thyroid nodule described as a TIRADS 5 category due to a nonparallel orientation. The patient looked closely in the medical literature, where he found that the ATA guideline gives a 70-90% and the ETA system a 26-78% cancer probability for TIRADS category 5 nodules. He said he came to the order only to have another doctor confirm that the nodule was indeed TIRADS 5 category.
Palpation: no abnormality.
Laboratory test: TSH 1.49 mIU/L.
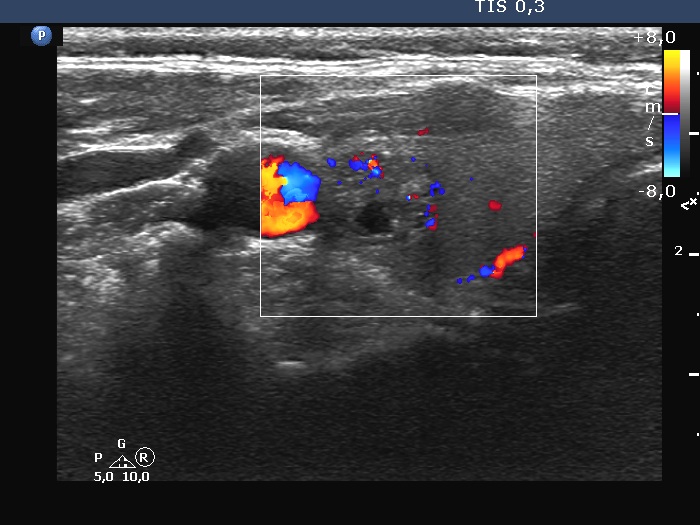
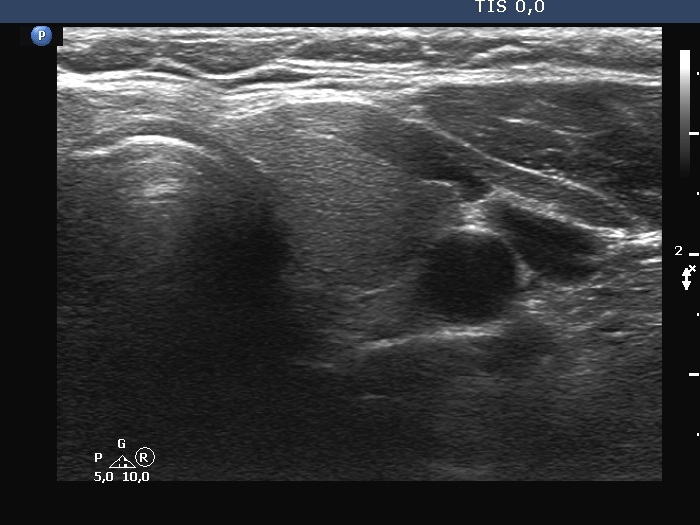
Ultrasonography. The thyroid was echonormal. There was a dominantly solid nodule in the right lobe. The lesion showed back wall cystic figures caused by posterior enhancement and nonparallel orientation. The depth of the nodule was 12 mm while the width was 10 mm.
We told the patient that although the lesion did indeed prove to be TIRADS 5, there was minimal if any risk of malignancy based on the ultrasound pattern. The patient said that considering what he was reading, he would only be reassured if the nodule was removed. I failed to convince him that a cytological examination would most likely give a reassuring result. He also withdrew from cytology.
By exploring the problem, we managed to make the patient uncertain about the justification for the surgery and temporarily postponed the decision regarding the surgery. Unfortunately, I'm not convinced this was really in the patient's best interest. Three months later, he came back for inspection much earlier than proposed. In the meantime, he even asked for the opinions of two other experts who also discouraged him from the surgery. Apparently, at our second appointment, the patient was much more anxious than at our first visit. The nodule, of course, showed no change. I suggested that if this problem causes such anxiety, it may still be worthwhile to have surgery.
Comments.
-
According to the classification of the European Thyroid Association, the lesion should be classified as TIRADS 5 while cannot be categorized on the guideline of the American Thyroid Association. The latter system cannot handle isoechoic lesions presenting suspicious findings.
-
People's decisions are not solely driven by rational considerations. Procedures can only be interpreted by a physician experienced in the field. He or she is expected to evaluate a problem in a complex way. We forget that the layman has the same access to what we read, but obviously is not able to make a complex assessment, he or she often snatches out a piece of data. It would be worthwhile to take the above into account when publishing the guidelines, and to note, for example, that the evaluation of the data requires special expertise.