
|
|
Teamwork - case 2223
|
|



Clinical presentation: A 9-year-old girl was referred for aspiration cytology. She had been treated for hypothyroidism for three months. On ultrasound a suspicious nodule was detected but FNA was non-diagnostic.
Palpation: no abnormality.
Laboratory tests: TSH 3.14 mIU/L on daily 50 microgram levothyroxine.
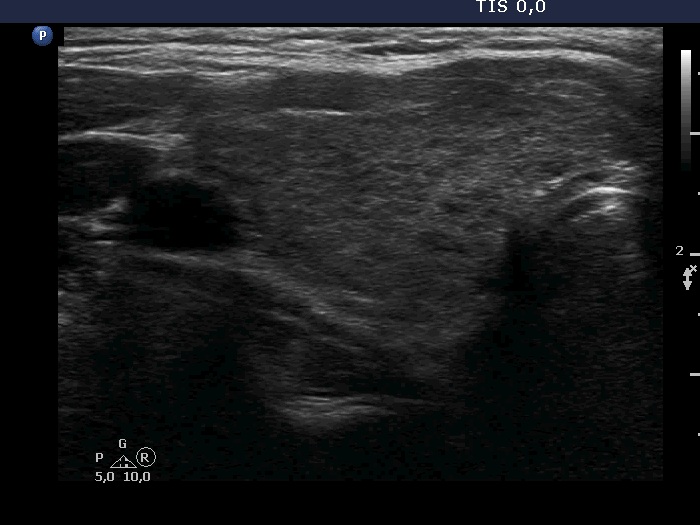
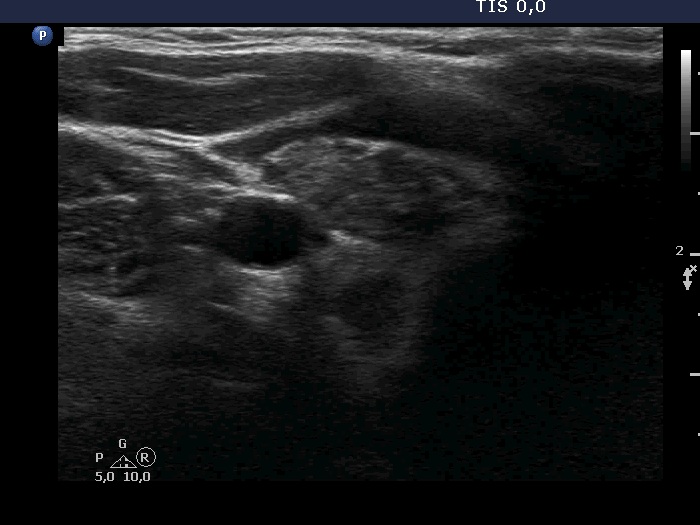
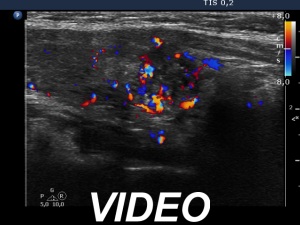
Ultrasonography. The thyroid was minimally hypoechoic and had more hypoechoic areas. There was a more hypoechoic nodule in the lower pole of the right lobe. The lesion has irregular, lobulated margins and numerous microcalcifications. A few microcalcification were found outside the core of the tumor. The intranodular vascularization was irregularly increased.
Cytological pattern corresponded to Hashimoto's thyroiditis. A few non-metaplastic cells contained inclusions.
A combined ultrasound-cytological diagnosis was Hashimoto's thyroiditis and papillary cancer.
Histopathology disclosed papillary cancer and Hashimoto's throiditis.
Comments.
-
The ultrasound presentation of the nodule is very suspicious for papillary cancer. Indeed, this pattern is almost diagnostic.
-
Although the cytological pattern itself was not fully decisive, we could give a decisive, combined ultrasound-cytological diagnosis.