
|
|
Teamwork - case 201
|
|









First examination (1st row of images)
Clinical presentation. A 45-year-old man was referred for cytology of a discrete lesion found on ultrasound examination. The patient had been treated for hypothyroidism for several years.
Palpation: no abnormality.
Hormonal evaluation: TSH 2.19 mIU/L on daily100 microgram levothyroxine.
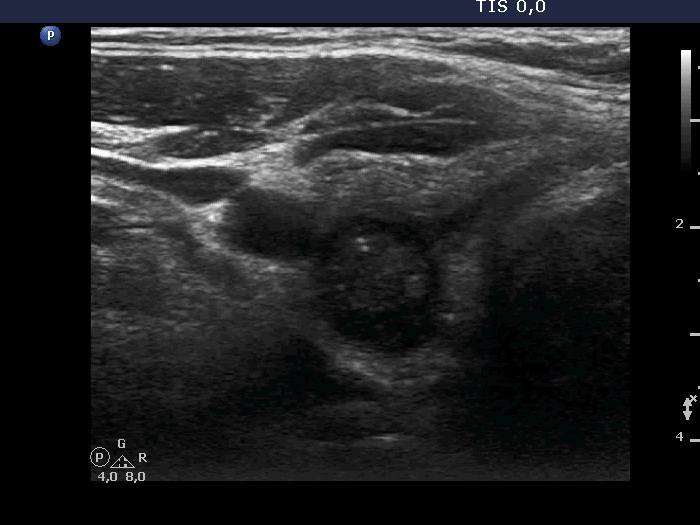
Ultrasonography. The thyroid presented the typical focal form of lymphocytic thyroiditis, it had numerous, tiny, hypoechoic areas. There was a more regularly shaped and larger lesion in the dorsal part of the right lobe. This lesion had at least one punctate echogenic focus.
Aspiration cytology of the lesion resulted in Hashimoto's thyroiditis.
Second examination 2 years later (2nd row of images)
Clinical presentation. The patient had no complaints. The endocrinologist colleague noticed a significant increase in the size of the nodule on repeat ultrasound and he sent the patient for a repeat FNA.
Palpation: no abnormality.
Ultrasonography. The pattern was essentially the same. The only difference concerned the lesion in the dorsal part of the right lobe which clearly increased in size. Moreover, it became more obvious that the lesion had microcalcifications.
Aspiration cytology of the lesion resulted in Hashimoto's thyroiditis.
Suggestion: In agreement with the referring physician, surgery was proposed because there was a suspicion of thyroid cancer despite the negative cytology.
Histopathology disclosed Warthin-like variant of papillary cancer. and Hashimoto's thyroiditis.
Comments.
-
It is worth noting that the FNA of a nodule which is covered with relatively deep ventral non-nodular tissue, necessarily has limitations. Since the success of the non-aspiration sampling technique, we know that the needle collects material from the tissue it passes through without aspiration. Of course, we try to get a sample from the lesion itself by making aspiration only when the needle reached the nodule, but if the needle is blocked during its route to the nodule, this is not always successful. In this patient we made 5 aspirations on 2 occasions. All of the smears showed only Hashimoto's thyroiditis.
-
The discrete lesion showed see features on which a different pathology could be suspected: in contrast with other hypoechoic smaller areas, the larger lesion was more hypoechoic, had a more regular shape and had microcalcification.
-
Considering above described circumstances and the significant increase in size, it seemed to be rational to suggest surgery.