
|
|
Case 1577
|
|




Clinical presentation: A 38-year-old woman was referred for aspiration cytology. Previous ultrasound reports were equivocal whether the thyroid had nodules or not. This caused anxiety to the patient. The patient had been treated for hypothyroidism for three years.
Palpation: no abnormality.
Laboratory tests: TSH 1.82 mIU/L on daily 75 microgram levothyroxine
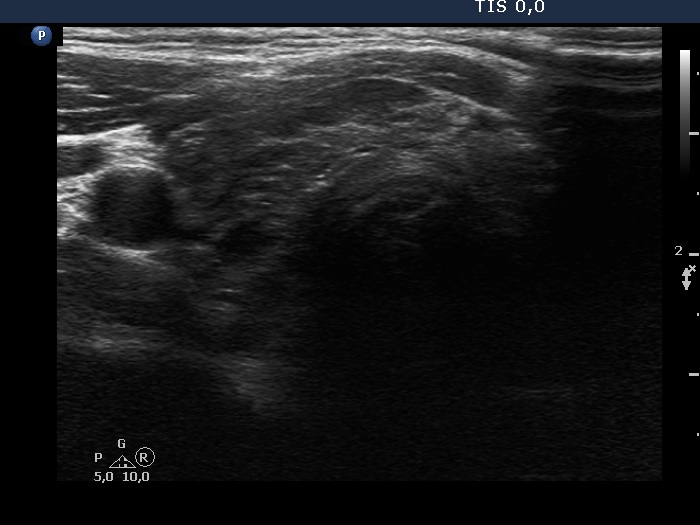
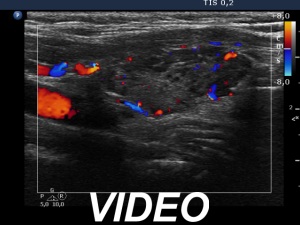
Ultrasound. The thyroid has echonormal and hypoechoic areas. The echogenicity index was greater than 50%. There was a relatively larger echonormal areas in the central-dorsal part of the left lobe. This was less influenced by the underlying thyroiditis. Nevertheless, neither this nor other areas in the thyroid corresponded to true nodules. the so-called honeycombing pattern, i.e., there were numerous small hypoechogenic areas within an echonormal background. The largest hypoechogenic area was misinterpreted as a nodule on previous ultrasound examination. This field was simply the largest of the similarly hypoechogenic parts of the thyroid. Considering the body mass, the thyroid was not enlarged.
Aspiration cytology resulted in Hashimoto's thyroiditis.
Comment.
-
It is worth analyzing the presentation of the left lobe. The pattern demonstrates how the thyroiditis infiltrates the normal parenchyma. In this case, the interpretation of echonormal areas should not be a major concern, these are not true nodules.
-
Cytology was performed solely for psychic reasons. A reassuring cytological finding is for a lifetime and prevents unnecessary anxiety in the patient later on. If this is not done, in each case one interpretation (no nodule in the thyroid gland) is opposed to another interpretation (there is a nodule in the thyroid gland).