
|
|
Case 2007/only for Videolibrary and Exam/ |



Clinical data: A 15-year-old girl was referred for aspiration cytology. She has been treated for hypothyroidism for 9 months when ultrasound revealed a suspicious nodule.
Palpation: a firm nodule in the isthmus.
Laboratory tests: TSH 3.74 mIU/L on daily 50 microgram levothyroxine. The aTPO was > 1300 U/mL at the time of the diagnosis of hypothyroidism.
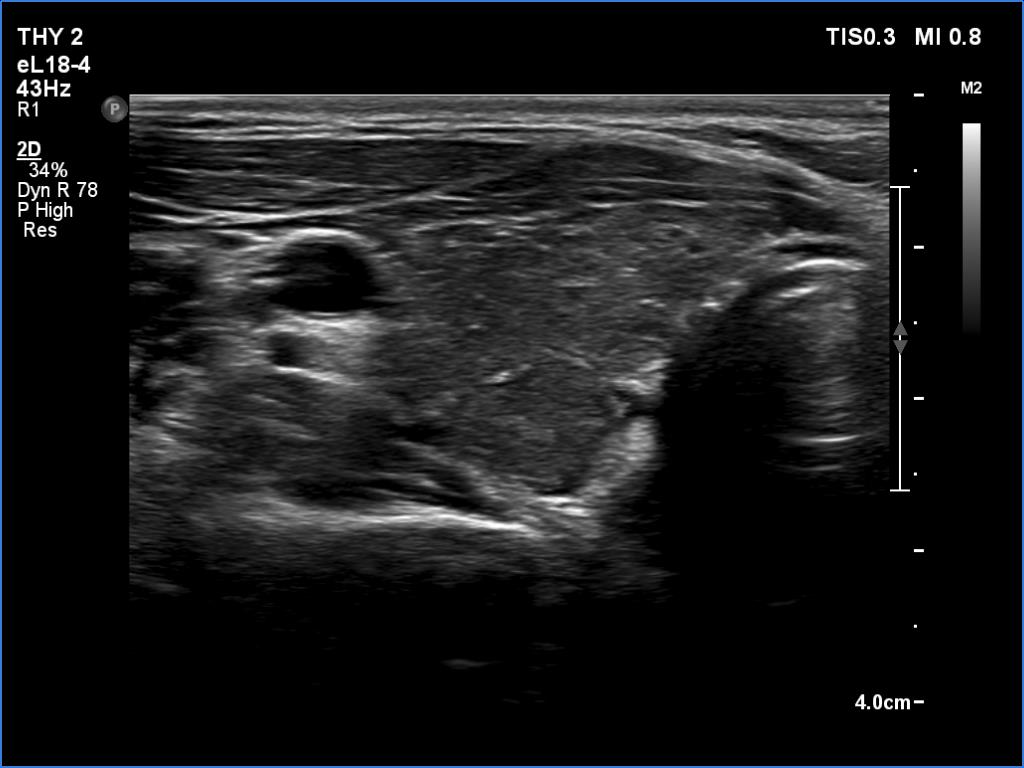
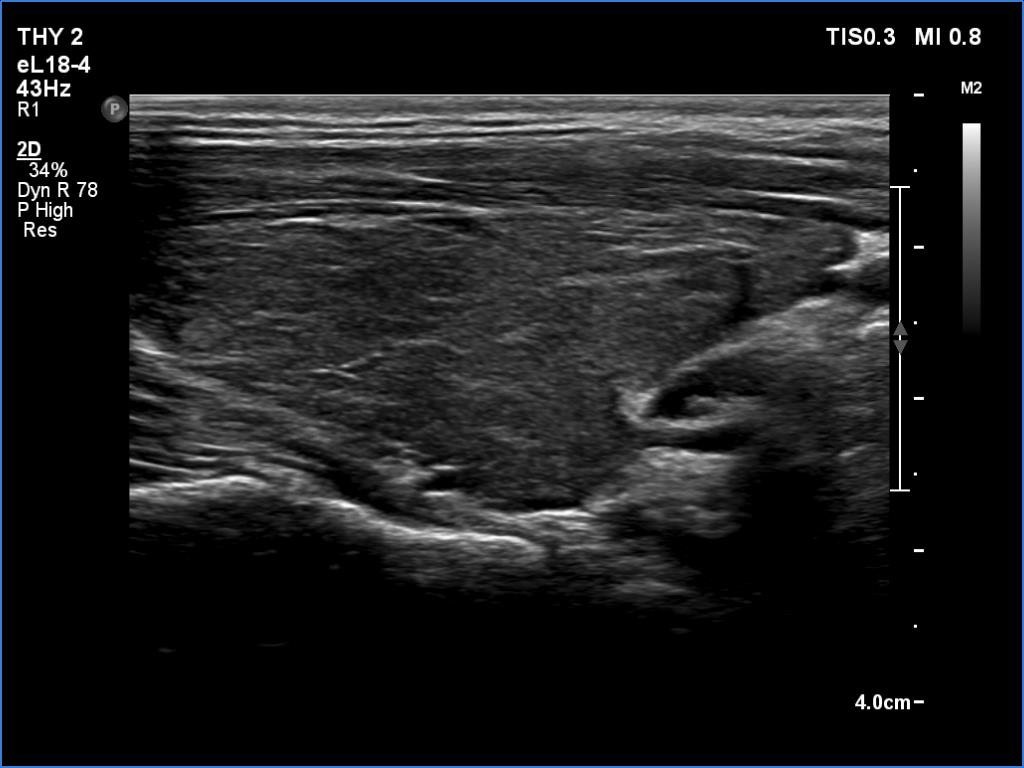
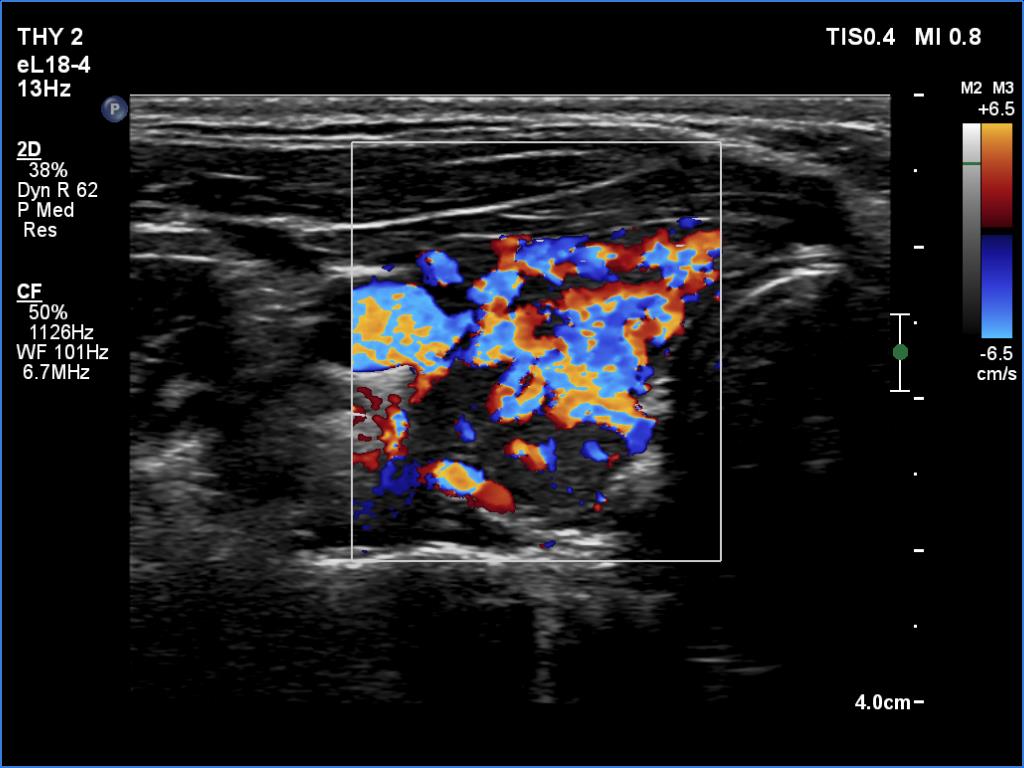
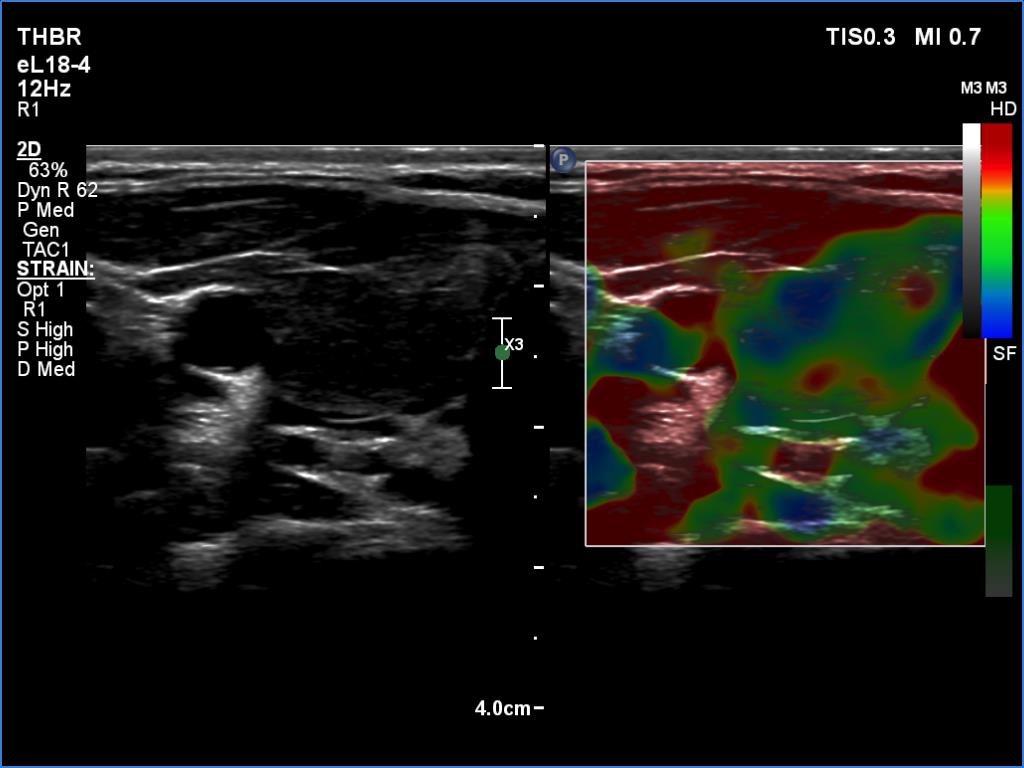
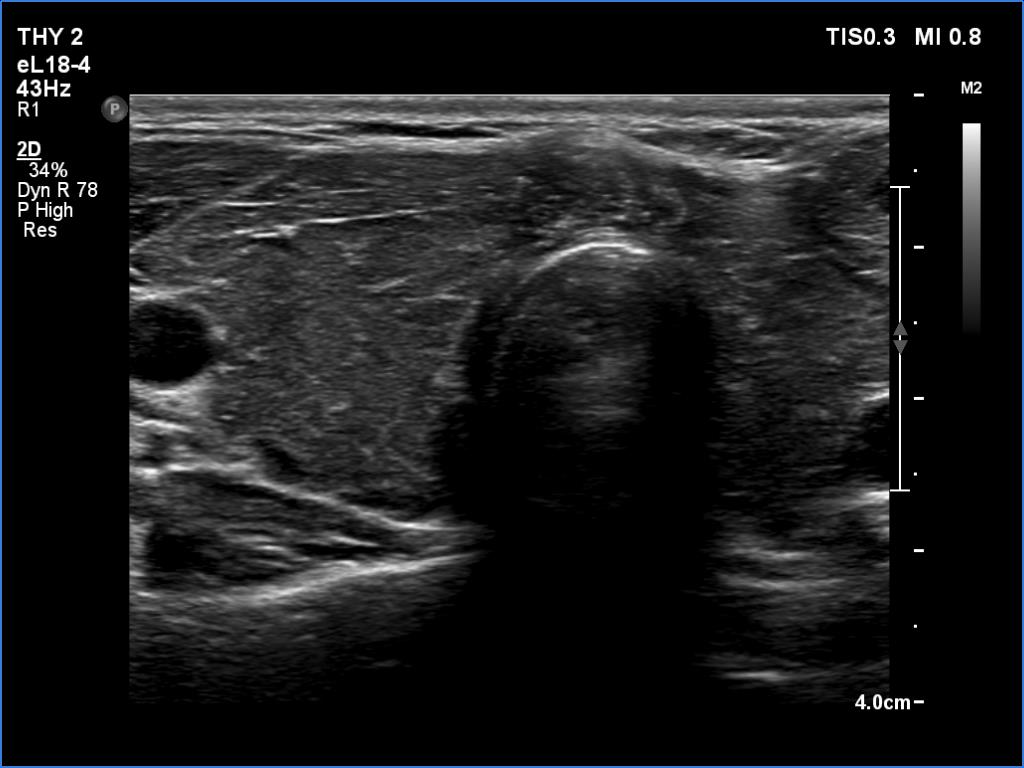
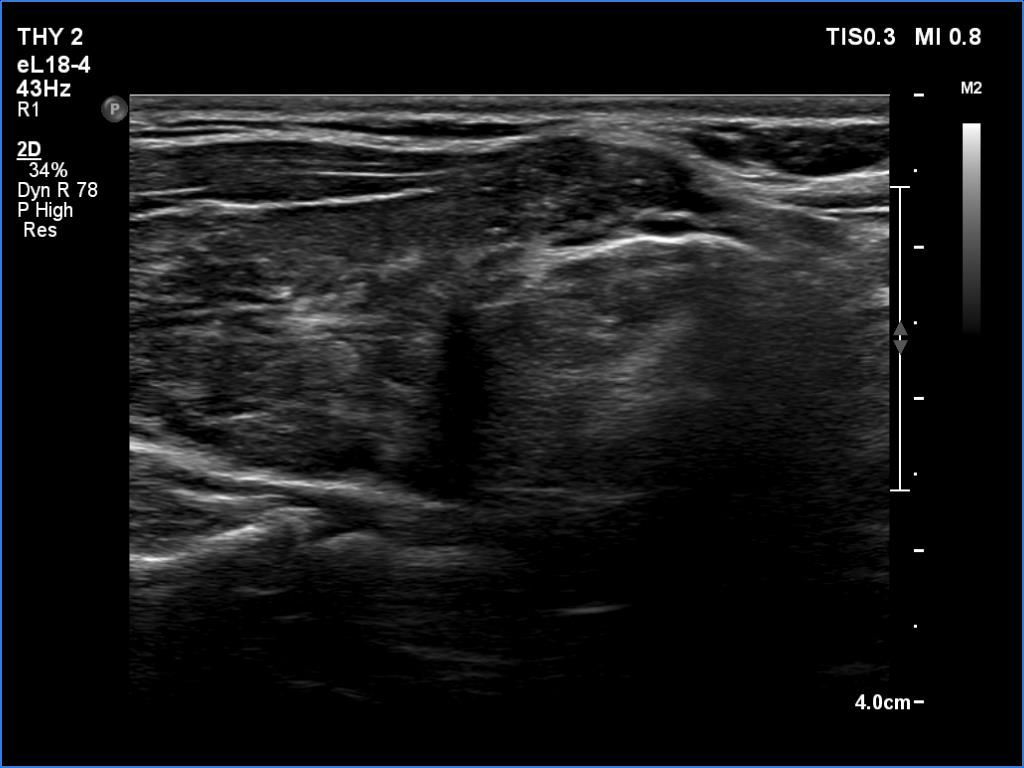
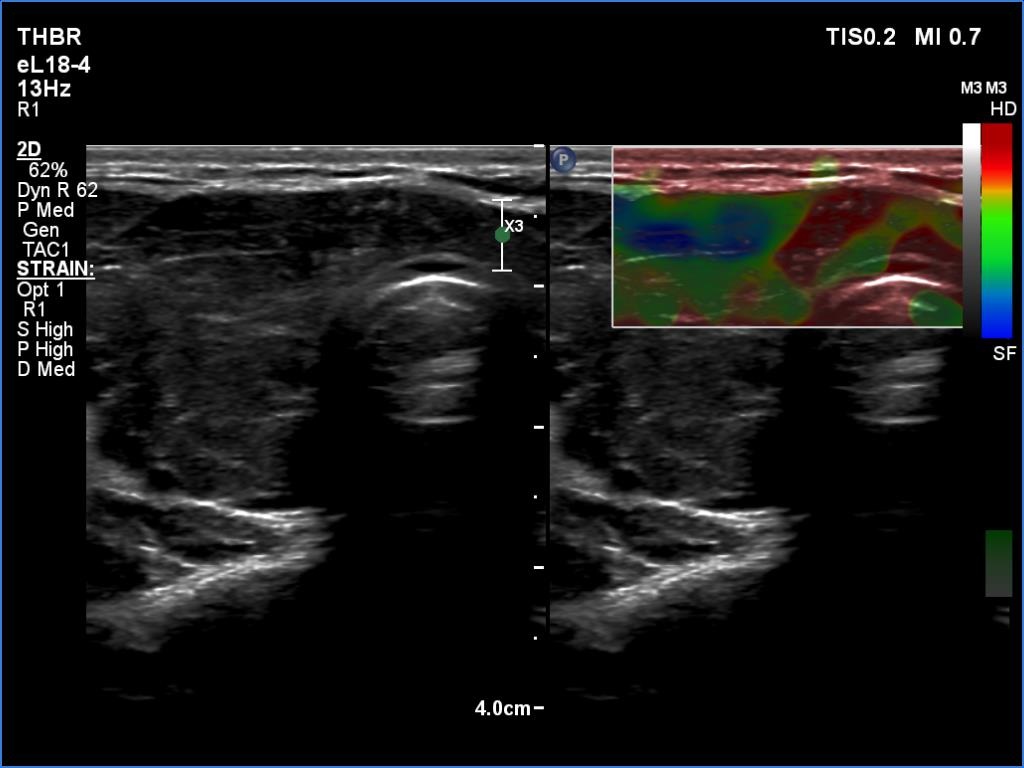
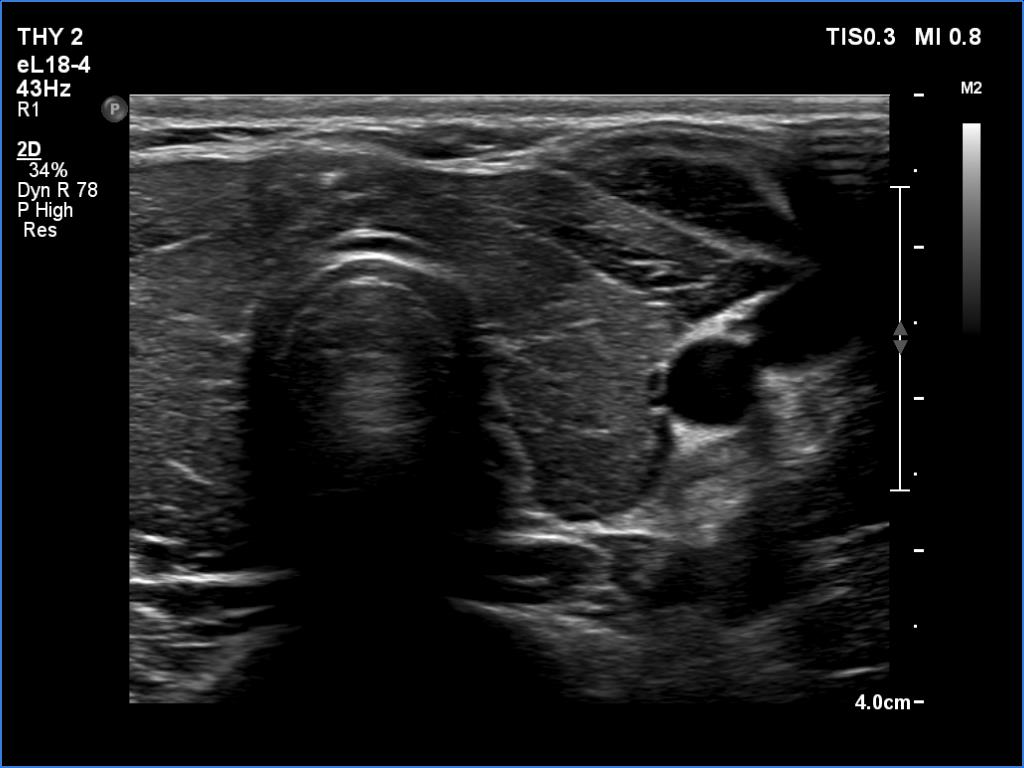
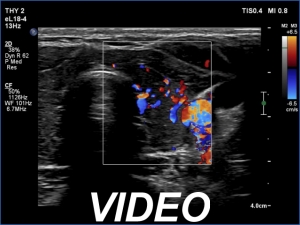
Ultrasonography. The thyroid was moderately hypoechoic and inhomogeneous. There was a deeply hypoechoic lesion in the isthmus which presented microcalcifications. Compared with the extranodular tissue, the nodule was much less vascularized on Doppler and microflow imaging but was harder on elastography.
Cytology resulted in papillary carcinoma.
We suggested a right lobectomy and isthmusectomy because it seemed to be likely that the patient has a T1 tumor.
Right lobectomy and isthmusectomy was performed. Histopathology disclosed a T1a papillary cancer and Hashimoto's thyroiditis in the extranodular tissue.
Comments.
-
Compared with nodules found in either lobe, the ultrasound signs of extrathyroidal spread are even more controversial in a nodule which is located in the isthmus. Such nodules necessarily present abutting and bulging contours.
-
There were two conditions which favored that the discrete lesion in the isthmus is a true nodule and not a more active focus of the underlying Hashimoto's thyroiditis. Firstly, the palpation which itself was suspicious of a cancer. Second, the presence of microcalcifications. It is worth comparing the similarly deep hypoechoic areas in the left lobe with the presentation of the cancer focus.