
|
|
Thyroid cancers - case 1202
|
|








First examination (first row of images)
Clinical data: A 45-year-old woman was referred for repeat cytology. A multinodular goiter was diagnosed on evaluation of weight gain. A suspicious nodule having microcalcifications was described in the isthmus and cytology resulted in Bethesda 3, atypia of unknown significance. On the cytological report even a C-cell origin was raised. Calcitonin test was negative 1.38 pM/L (normal range 0-5.33).
Palpation: a not firm nodule in the left lobe.
Laboratory tests: TSH 2.13 mIU/L.
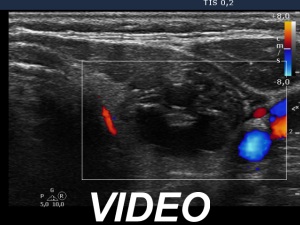
Ultrasonography. The thyroid was echonormal. There was a moderately hypoechoic nodule in the right lobe. The lesion presented halo and both perinodular and intranodular blood flow. The dimensions were 18x11x20 mm, width, depth, length, respectively. The left lobe had a cystic nodule which presented back wall cystic figures but not microcalcifications. The dimensions were 18x16x27 mm, width, depth, length, respectively.
Cytology was performed form both nodules and resulted in benign lesion and benign cystic-colloid goiter, right and left nodule, respectively.
Suggestion: ultrasound in a year.
Second examination 6 years later (second row of images)
Clinical data: The patient did not show up at the proposed checkup but this time she requested a repeat examination because she noticed that the nodule in the left lobe has increased.
Palpation: A firm nodule in the left side of the isthmus.
Laboratory test: TSH 1.06 mIU/L.
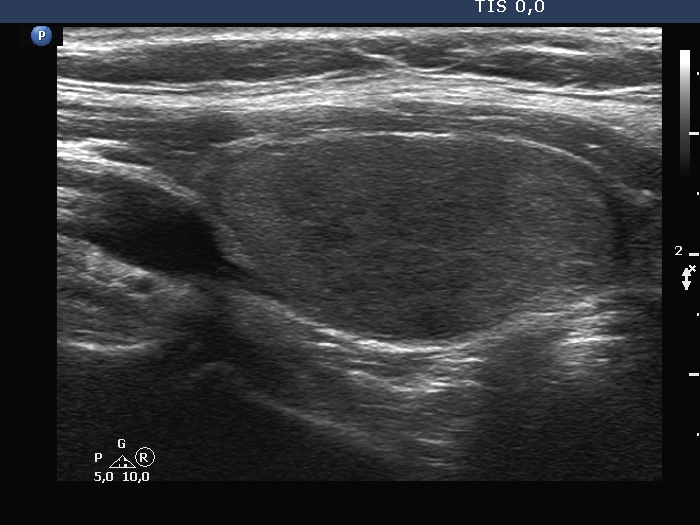
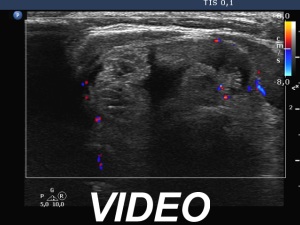
Ultrasonography. Both previously described nodules have significantly increased in size. The dimensions of the right nodule were 25x17x36 mm, width, depth, length, respectively.
The nodule, which was previously described in the left lobe, seemed to be located in the isthmus. The dimensions of this lesion were 36x18x40 mm, width, depth, length, respectively. Except for the significant increase in size, the pattern of the nodules remained unchanged. Several small, hypoechoic discrete lesions were found in the left lobe.Cytology was performed form both nodules and resulted in follicular tumor and benign cystic-colloid goiter, right and left nodule, respectively. The cyst could not be emptied, only a small amount of brown fluid could be aspirated.
Total thyroidectomy was performed. Histopathology disclosed minimally invasive follicular cancer and benign hyperplastic nodules, right nodule and other nodules, respectively.
Comments.
-
The ultrasound presentation of the nodule in the left lobe or in the left side of the isthmus was typical of a benign cystic lesion. The back wall figures were misinterpreted as microcalcifications.
-
Depending on the positioning of the tranducer, nodules located at the isthmic part of a lobe can be projected as it were within the lobe or in the isthmus.
-
We reviewed the smear gained from the malignant nodule, but our diagnosis was correct. The issue was that we performed only one aspiration from the nodule at the first visit because we focused on the nodule which was falsely described as suspicious.
-
It is worth noting the significant increase of the malignant nodule, the volume increased 3.9-fold over 6 years. The increase of a cystic nodule has limited relevance, this was caused by the accumulation of the fluid.
- In my own practice, less than half of the nodular patients show up at the time of the proposed checkup.