
|
|
Study on 100 consecutive patients with thyroid nodule - case 021
|
|





Clinical presentation: A 39-year-old woman was referred for evaluation of a thyroid nodule which was discovered on screening.
Palpation: no abnormality.
Functional state: TSH 2.67 mIU/L. aTPO < 28 U/ml, ahTG 0,9 U/l on daily 50 microgram levothyroxine.
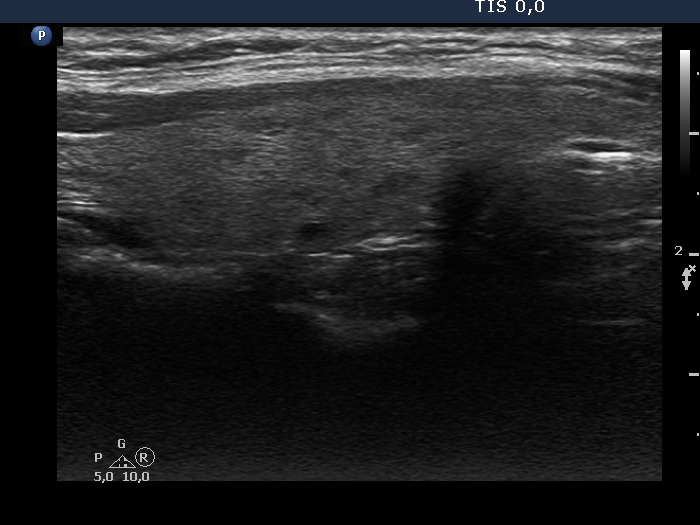
Ultrasonography. The thyroid was echonormal and had tiny, moderately hypoechoic areas. The echogenicity index was around 10%. There was a dominantly hypoechoic, heterogeneous nodule in the left lobe. The lesion presented various echogenic figures, including microcalcifications and amorphous hyperechoic patches.
We extended the laboratory tests with aTPO which proved to be > 1300 U/mL and calcitonin which resulted in 1.56 pM/L (normal value < 5.9 pM/L).
Cytology resulted in Bethesda III, atypia of unknown significance category. (There were atypical cell groups with nuclear crowding. Several nuclei had grooves but no inclusion was found.)
We suggested follow-up with repeat FNA. The patient first agreed with the proposal. However, a few weeks later, she visited again and said that considering the risk of cancer, she definitely wants the nodule to be removed. I said again that if she takes the follow-up, there is no risk if the surgery is not done now, but even a year or two later. She said she does not want that uncertainty and her GP was on the same opinion.
Histopathology disclosed an encapsulated papillary cancer. The tumor spread beyond its capsule but remained within the thyroid. Hashimoto's thyroiditis was found in the extranodular tissue.
Comments.
-
It is difficult to classify all intranodular echogenic figures.
- This case study points to several weaknesses of the management of thyroid patients.
First, thyroid specialists are aware that for a well-differentiated cancer, there is no detectable harm from having surgery a few years later. However, it is very difficult to convince the patient of this if we do not receive full support from other colleagues for it. A thyroid specialist will sooner or later find that non-expert colleagues are different from treating a thyroid problem such as an oncological or cardiological problem. For the latter, it is very rare to question the opinion of a cardiologist or oncologist, while this is quite common in the case of the thyroid gland. Given that here the body's less aggressive, non-benign tumor is in question, a general awareness, it will necessarily show worse odds than the real situation. Many times, a simple metacommunicative gesture is enough to make the patient feel at risk. The effect of a half-hour, thorough discussion and information with an expert can be negated by a single ambiguous remark or gesture by a non-expert colleague.
The issue is that most papillary cancers do not behave malignant. A long time ago, it would be time to call this tumor or at least certain some forms of it the way it behaves. The name cancer is quite simply misleading. For most patients, the term 'cancer' makes rational decision difficult, and often impossible.