
|
|
Study on 100 consecutive patients with thyroid nodule - case 042 |
|















First examination (first row of images)
Clinical data: A 53-year-old woman was referred for evaluation of a nodule discovered on ultrasound screening. She had no complaints.
Palpation: there was a moderately firm nodule in the left thyroid.
Functional state: euthyroidism with TSH 1.06 mIU/L.
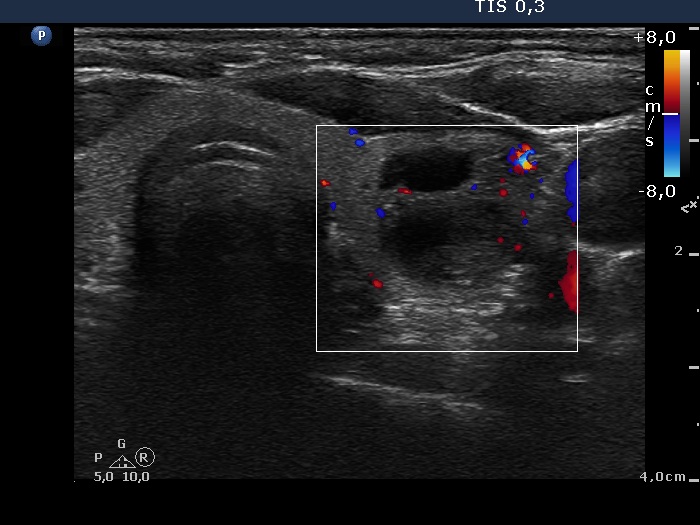
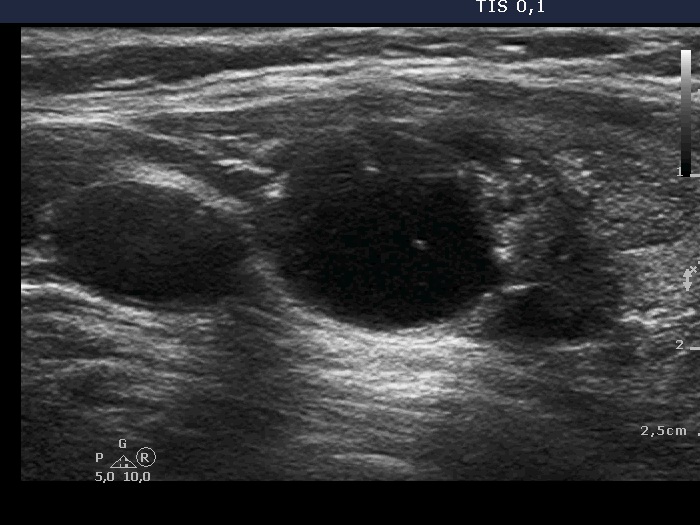
Ultrasound. The thyroid was echonormal. There was a mixed nodule in the ventral part of the left lobe. The lesion presented a moderately hypoechogenic solid part and different types of hyperechogenic figures including several caused by posterior back wall enhancement, comet-tail artifacts and non-specific figures corresponding to connective tissue.
One mL brown cystic fluid was aspirated. Cytological report: not diagnostic, cystic lesion.
A repeat cytology was advised 6 to 12 months later.
Second examination (second and fourth rows of images)
Clinical data: The patient had no complaints. She came to routine follow-up.
Palpation: unchanged.
Functional state: euthyroidism with TSH 0.85 mIU/L.
Ultrasound remained unchanged. Compared with the previous examination the nodule has not increased in size.
Suggestion: ultrasound in three years.
Third examination (third rows of images)
Clinical data: The patient had no complaints. Ultrasound was performed for a month in another hospital and the radiologist told the patient that her nodule is highly suspicious because of the presence of microcalcifications. The lesion was categorized as a TIRADS 5 lesion.
Palpation: unchanged.
Functional state: euthyroidism with TSH 0.85 mIU/L.
Ultrasound. There was one important change compared with the previous exams. A lobulation has appeared at the lower part of the lobe. This portion was solid and had punctate echogenic foci.
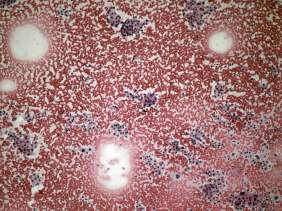
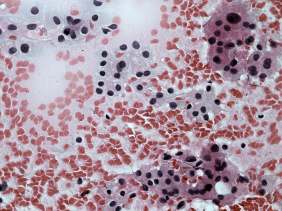
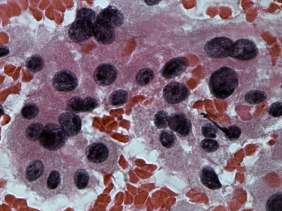
Aspiration cytology resulted in follicular proliferation.
Combined ultrasound-cytological diagnosis was benign follicular proliferation.
Follow-up was advised, however the patient decided to go on surgery because of the ultrasound report of the colleague.
A total thyroidectomy was performed and histopathology disclosed benign hyperplastic nodules.
Comments.
-
The cytological pattern itself is on the verge of a clearly benign proliferation and a follicular tumor: there was no colloid in the background and the ratio of isolated follicles was greater than in usual cases of a hyperplastic nodule. On the other hand, the presence of pyknotic nuclei and degenerative forms as well the heterogeneous pattern suggested a non-tumorous origin.
-
The ultrasound presentation was also remarkable. First, there are no signs of a capsule which decreases the likelihood of a follicular tumor to less than 5%. Second, the nodular area is composed of multiple discrete lesions which itself is a relatively specific sign of a hyperplastic nodule (see video).
-
The interpretation of tiny hyperechogenic granules is not always unequivocal and non-specific hyperechogenic granules are frequently misinterpreted as microcalcifications.
-
The TIRADS categorization shares several inherent problems. To describe a nodule on the ultrasound report as moderately suspicious or highly suspicious can cause more harm than all the system's benefit. Be aware that a patient is a human being with his or her distress caused by the medical examination itself. Why further increase the anxiety? His or her nodule will be soon aspirated if necessary.
-
This case illustrates the issue of differential diagnostic or intranodular figures: granules occurring in the presence of connective tissue, colloid crystals and figures caused by posterior back wall enhancement all may be misinterpreted as microcalcifications as happened in this patient.
-
The above listed points may be disputed but we think that considering all of the conditions described above, the choice of a total thyroidectomy was a failure.